 Gabriella Gálffy
Gabriella Gálffy Éva MoróczRéka KorompayRéka Hécz
Éva MoróczRéka KorompayRéka Hécz Réka Bujdosó
Réka Bujdosó Rita PuskásTímea LovasEszter GáspárKamel YahyaPéter Király
Rita PuskásTímea LovasEszter GáspárKamel YahyaPéter Király Zoltán Lohinai*
Zoltán Lohinai*- Pulmonology Hospital Törökbálint, Törökbálint, Hungary
The complex therapeutic strategy of non-small cell lung cancer (NSCLC) has changed significantly in recent years. Disease-free survival increased significantly with immunotherapy and chemotherapy registered in perioperative treatments, as well as adjuvant registered immunotherapy and targeted therapy (osimertinib) in case of EGFR mutation. In oncogenic-addictive metastatic NSCLC, primarily in adenocarcinoma, the range of targeted therapies is expanding, with which the expected overall survival increases significantly, measured in years. By 2021, the FDA and EMA have approved targeted agents to inhibit EGFR activating mutations, T790 M resistance mutation, BRAF V600E mutation, ALK, ROS1, NTRK and RET fusion. In 2022, the range of authorized target therapies was expanded. With therapies that inhibit KRASG12C, EGFR exon 20, HER2 and MET. Until now, there was no registered targeted therapy for the KRAS mutations, which affect 30% of adenocarcinomas. Thus, the greatest expectation surrounded the inhibition of the KRAS G12C mutation, which occurs in ∼15% of NSCLC, mainly in smokers and is characterized by a poor prognosis. Sotorasib and adagrasib are approved as second-line agents after at least one prior course of chemotherapy and/or immunotherapy. Adagrasib in first-line combination with pembrolizumab immunotherapy proved more beneficial, especially in patients with high expression of PD-L1. In EGFR exon 20 insertion mutation of lung adenocarcinoma, amivantanab was registered for progression after platinum-based chemotherapy. Lung adenocarcinoma carries an EGFR exon 20, HER2 insertion mutation in 2%, for which the first targeted therapy is trastuzumab deruxtecan, in patients already treated with platinum-based chemotherapy. Two orally administered selective c-MET inhibitors, capmatinib and tepotinib, were also approved after chemotherapy in adenocarcinoma carrying MET exon 14 skipping mutations of about 3%. Incorporating reflex testing with next-generation sequencing (NGS) expands personalized therapies by identifying guideline-recommended molecular alterations.
Introduction
In recent years, there has been an expansion in the treatment options of non-small cell lung cancer (NSCLC) with the advent of targeted therapies and immuno-oncology therapies [1, 2]. Lung tumors are heterogeneous, with distinct oncogenic drivers and tumor microenvironments. Tumor evolution results in distinct organ site metastases representing intratumor heterogeneity and the ongoing development of resistance mutations [3]. Recent advancements in cost-effective parallel high-throughput molecular diagnostics might drive personalized therapy beyond adenocarcinoma subtypes associated with the most targetable genetic alterations [3]. Prior to precision medicine, patients were treated uniformly without considering the differences in clinicopathological characteristics and genetic backgrounds of different patients. The careful selection for upfront treatments of brain metastases (BM) might be detrimental to outcomes [1, 2]. Now, it is clear that patients with oncogenic driver alteration-positive NSCLC are associated with better outcomes treated with frontline targeted therapy compared to chemotherapy and anti-Programmed death (anti-PD) immunotherapy [1, 2]. Today, the right choice of molecular diagnostics is increasingly important, following the careful classification of pathological diagnostics. While stand-alone single gene assays remain valid, increasing requirements for synchronous testing for multiple targets make massive parallel sequencing technology the preferred option [2]. DNA sequencing is the standard for mutation detection, and RNA sequencing is an emerging option for fusion gene detection. EGFR, ALK, and ROS1 alterations are common for young female non-smokers with adenocarcinoma [4]. While ALK and ROS1 mutations do not show ethnic prevalence, one can observe a four times elevated EGFR prevalence in the Asian population compared to the Western population [4]. KRAS and MET mutations occur in older age populations with smoker status and adenocarcinoma. There is no clear gender preference, but a distinct excess of KRAS mutations in the Caucasian population is observable. It is widely accepted that KRAS mutation in lung cancer is smoking-associated, but it is only proven for G12C [5, 6]. BRAF mutations occur in smokers without age or ethical tendencies. The BRAF V600 mutations are detected with a higher incidence for females; other BRAF mutations have a higher incidence for the opposite sex. HER2 mutations have a higher likelihood for female and never-smoker patients [4]. In contrast to the known associations of genetic alteration with clinicopathological characteristics, according to the latest guidelines, molecular testing is now the standard for advanced-stage adenoma-carcinoma-containing cancers independent of sex, ethnicity, or smoking [2]. Therefore, histology assessments are key in clinical practice, with a cautious interpretation of mixed histology specimens and NSCLC not otherwise specified (NSCLC NOS) because molecular testing is recommended for non-squamous NSCLC cases. Testing is also recommended for NSCLC cases below 50 years of age and all kinds of tobacco in patients who quit smoking more than 15 years ago, or in never (<100 cigarettes overall) or former light (≤15 6 pack-years) or long-time ex-smokers (quit >15 years ago). Importantly, the presence of any adenocarcinoma component in a biopsy specimen that is otherwise squamous should trigger molecular testing. Accordingly, cautious minimization of tissue slides used for immunohistochemistry (IHC) stainings and preserving material for molecular testing is critical. Oncogenic driver tests usually follow the Programmed death-ligand 1 (PD-L1) IHC testing for non-squamous cases. The present review summarizes the available data on targeted therapy strategies in treating NSCLC (Figure 1). A particular focus is given to central nervous system (CNS) activity that is detrimental in the era of better control of oligoprogressive disease. Additionally, for optimal treatment outcomes, we highlight the role of distinct molecular analyses based on accurate guideline-based histology classifications to avoid excluding patients from therapy. Nevertheless, the emergence of early-stage targeted therapies extends molecular testing beyond advanced-stage disease.
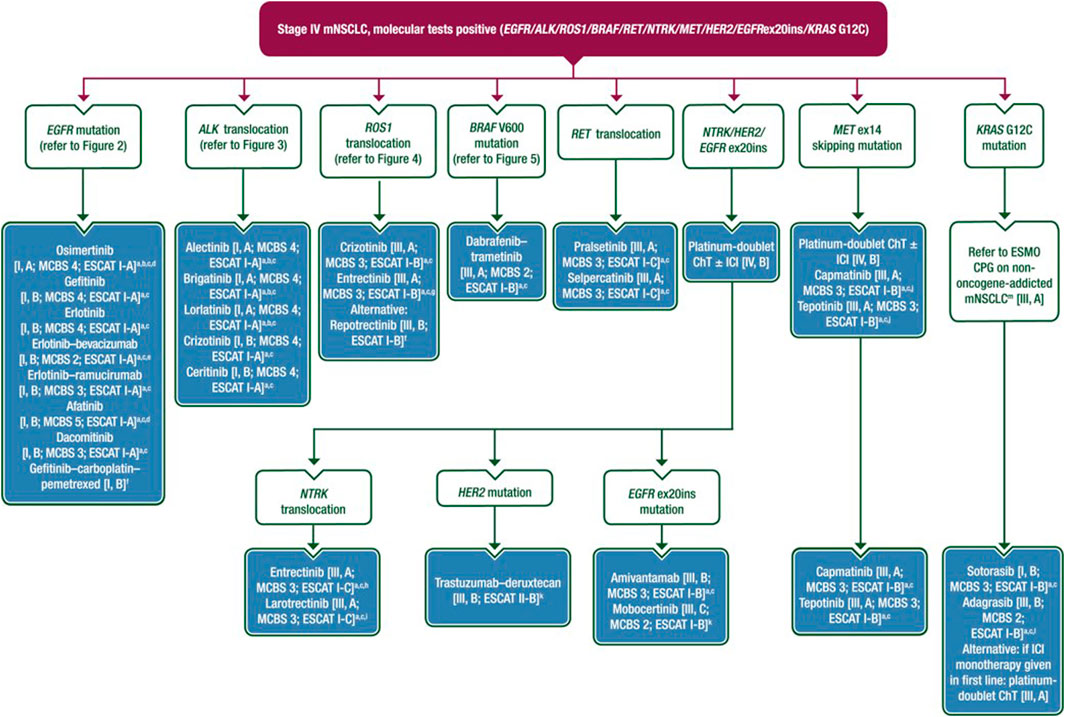
Figure 1. Treatment recommendation for stage IV mNSCLC based on the ESMO 2023 guideline [1].
Adjuvant osimertinib therapy in the treatment of NSCLC
As adjuvant treatment in NSCLC, osimertinib is the first targeted therapy approved based on the ADAURA trial. The ADAURA trial enrolled stage I/B -III/A patients with classical epidermal EGFR mutations (ex19del/L858R) who underwent complete tumor resection [7]. Patients were allowed to receive adjuvant chemotherapy before osimertinib, and optionally, they were allowed to start osimertinib therapy after surgery. According to the 1:1 randomization, the study group received osimertinib, and the other group received a placebo at a planned interval of 3 years. The primary endpoint was disease-free survival (DFS) in stage II/IIIA patients. DFS in the osimertinib group compared to placebo showed a significant benefit (hazard ratio (HR): 0.23, 95% CI 0.18–0.30) median DFS was 65.8 months for the osimertinib compared to 21.9 months for the placebo arm [8]. Subgroup analysis (gender, age, race, stage, mutation type) revealed significant benefits in DFS. Adjuvant osimertinib also showed efficacy without cytotoxic chemotherapy, with a significant benefit in DFS (HR: 0.23), and osimertinib given followed by adjuvant chemotherapy showed a similar significant benefit in DFS (HR: 0.16) [8].
NSCLC with actionable EGFR mutations
The HER/Erb family epidermal growth factor receptor (EGFR) is a transmembrane tyrosine kinase (TK) receptor that stimulates cell proliferation, differentiation, survival, and motility through MAP kinase and PI3K signaling pathways [9]. Overexpression and increased activity of EGFR tyrosine kinase in non-small cell lung tumors were first described in 2004, which may result from mutation, deletion, or amplification of the tyrosine kinase coding region [10].
The mutation most commonly affects exons 18–21 and occurs in 10%–20% of the Caucasian population, predominantly in young, never-smoker women. In almost 90% of cases, a so-called “classical mutation” is encountered, a deletion of exon 19 or a point mutation of exon 21 (L858R). The exon 20 insertion is the third most common EGFR mutation, accounting for 4%–12% of all EGFR mutations, it is more common in women, non-smokers, and Asians and is associated with a worse prognosis. In addition to the exon 20 insertion mutation, the most common rare mutations include exon 18 G719X, exon 20 S768I and exon 21 L861Q, which occur in 1%–3% of cases and smoking history [11].
In locally advanced or metastatic non-small cell lung cancer, EGFR tyrosine kinase inhibitor (TKI) treatment is the recommended first-line therapy with confirmed actionable EGFR mutations. EGFR tyrosine kinase inhibitors are classified into three generations based on their appearance in chronological order. The first-generation includes the reversible binding agents gefitinib and erlotinib, the second-generation includes the irreversible ErbB/HER2 inhibitor afatinib and the EGFR/pan-HER inhibitor dacomitinib, while the third-generation is osimertinib. Since then, several studies have demonstrated the benefit of EGFR tyrosine kinase inhibitors in terms of tumor response, safety, quality of life, and progression-free survival (PFS) compared with conventional chemotherapy regimens [12].
First-generation reversible EGFR inhibitors
Pioneering in the treatment of adenocarcinoma patients, gefitinib, in its pivotal phase 3 IPASS trial, showed a significant benefit in progression-free survival [median PFS (mPFS) gefitinib 9.5 months vs. chemotherapy 6.3 months; HR 0.48, 95% confidence interval (CI) 0.36–0.64 p < 0.001] and tumor response [objective response rate (ORR) 71.2% v 47.3%, p = 0.0001], with good quality of life maintained [13].
The efficacy of erlotinib was analyzed in the OPTIMAL trial in Asia and the EURTAC trials in Europe [14, 15]. A significant difference was demonstrated in favor of erlotinib in terms of overall survival (OS) and tumor response compared to the standard platinum-based chemotherapy regimens (EURTAC mPFS erlotinib 9.7 months vs. chemotherapy 5.2 months; p < 0.0001; ORR 64% vs. 18%; p < 0.0001) (OPTIMAL mPFS erlotinib 13.1 months vs. chemotherapy 4.6 months; p < 0.0001; ORR 83% vs. 36%; p < 0.0001) (5,6). Although no benefit in overall survival was demonstrated, following these trials, both products were registered in the first-line setting for treating EGFR mutation-positive stage IIIB/IV non-small cell lung cancer.
It is now well known that the first-generation drugs are most commonly associated with skin side effects (rash, xeroderma, pruritus, and paronychia), diarrhea, fatigue, and elevation of liver function, typically AST/ALT. The most common cutaneous side effects are acneiform rash, dry skin, itching, and nail bed lesions, which are well controlled by topical or systemic antibiotic treatment (doxycycline). Diarrhea can be reduced by per os medication (appropriate dose of loperamide), with drug dose reduction if necessary. Once the side effects are resolved, the original dose is often restored. Compared with chemotherapy regimens, first-generation regimens have shown a much better side-effect profile and fewer serious (grade 3–4) adverse events [13, 15–18].
A vascular endothelial growth factor (VEGF) inhibitor, Ramucirumab plus erlotinib, showed increased PFS compared to placebo plus erlotinib arm in patients with untreated EGFR-mutated metastatic NSCLC (mNSCLC) [19]. Safety was consistent with the safety profiles of the individual compounds in advanced lung cancer.
Second-generation EGFR inhibitors
The second-generation EGFR tyrosine kinase inhibitors (afatinib and dacomitinib) are more potent EGFR and HER2 inhibitors, forming irreversible binding. The efficacy of afatinib was analyzed in LUX-lung studies. In the phase 2 LUX-lung 3 and LUX-lung 6 trials, afatinib showed significantly better tumor response and progression-free survival than platinum-based chemotherapy combinations (LUX-lung 3, mPFS for afatinib vs. chemotherapy, 13.6 months vs. 6.9 months; respectively, p = 0.0004; ORR, 56% vs. 23%; p = 0.001; respectively; LUX-lung 6, mPFS for afatinib vs. chemotherapy 11.0 months vs. 5.6 months; p < 0.0001; respectively, ORR 66.9% vs. 23%; p < 0.0001). [20, 21]. It should be noted that afatinib did not provide a benefit in OS in the overall patient group; however, in subgroup analyses, targeted therapy in patients with exon 19 deletion showed a significant benefit in overall survival (LUX-lung 3, OS for afatinib vs. chemotherapy 33.3 months 21.1 months respectively; LUX-lung 6, OS for afatinib vs. chemotherapy 31.4 months vs. 18.4 months, respectively). This benefit was not confirmed for point mutations [22]. Based on these studies, afatinib was registered as a first-line treatment for non-small cell lung tumors carrying EGFR mutations.
The LUX-lung 7 phase 2 trial comparing first- and second-generation EGFR tyrosine kinase inhibitors compared afatinib with gefitinib, where afatinib was shown to be superior in terms of progression-free survival (mPFS for afatinib vs. gefitinib, 11.0 months vs. 10.9 months; respectively, p = 0.017), however, the study did not show a significant benefit in terms of overall survival and more toxicity leading to dose reduction was observed when using the second-generation drugs [23]. A higher rate of G3-severe skin rash (9.4% vs. 3.1%) and G3 diarrhea (12.5% vs. 1.3%) was also observed in the afatinib group. Dacomtinib, also a second-generation irreversible EGFR and panHER inhibitor, was superior to gefitinib in first-line use in the ARCHER1050 phase 3 trial in terms of both PFS and OS [PFS for dacomitinib vs. gefitinib, 14.7 months vs. 9.2 months, respectively, p < 0.0001; median OS (mOS) dacomitinib vs. gefitinib, 34.1 months vs. 26.8 months, respectively], but again a less favorable side effect profile was observed with dacomitinib [24, 25].
Third-generation EGFR inhibitors and T790 resistance mutation
Acquired resistance to first- and second-generation drugs develops after 9–13 months, with a T790 resistance mutation affecting exon 20 being confirmed in 50%–60% of cases [26]. This has led to the development of third-generation therapies [26]. Osimertinib is a third-generation irreversible EGFR TKI that is also effective in the presence of T790 resistance mutations. The efficacy of the first mutation selective TKI was analyzed in AURA trials. In the AURA 3 phase 3 trial, compared with platinum-based chemotherapy, osimertinib showed a significant PFS benefit in T790 resistance mutation-positive, locally advanced or metastatic NSCLC (mPFS osimertinib vs. chemotherapy, 10.1 month vs. 4.4 months, respectively, p < 0.001) [27]. This was followed by the phase 3 FLAURA trial, which compared the efficacy of osimertinib with first-generation agents; osimertinib achieved a significant benefit in both progression-free and overall survival, with osimertinib providing an 8.8 months OS benefit, reducing the risk of death by 20% (mOS osimertinib vs. first-generation EGFR inhibitor, 38.6 months vs. 31.8 months; respectively, HR 0.80; 95% CI, 0.6410 .997; p = 0.046). The side effect profile was similar, but G3 side effects were less frequent with osimertinib [28]. The most common osimertinib-induced adverse events were acneiform rash, diarrhea, and paronychia, and a small percentage of cardiomyopathy (∼1.4%–2.4%), QT prolongation (2.7%), and interstitial lung disease (ILD) (3.3%) were also described [29]. After 3 years of follow-up, 28% of patients received osimertinib, compared with only 9% in the comparator group. Notably, first-line osimertinib reduced the risk of CNS progression by 52% (HR, 0.48; 95% CI, 0.260.86; p = 0.014) and fewer de novo CNS metastases were recorded [30]. The importance of these results is demonstrated by the fact that 10%–30% of patients with NSCLC develop CNS metastases, which are associated with a worse prognosis and worse survival. EGFR mutations are present in 40%–60% of non-small cell lung tumors affecting the central nervous system, and the risk of central nervous system metastasis is higher in the presence of EGFR mutations, making the concentration of each drug in cerebrospinal fluid a key determinant. First- and second-generation drugs have limited brain penetration, while osimertinib rapidly crosses the blood-brain barrier (BBB) and reaches higher concentrations. Osimertinib, which has the best efficacy and most favorable side-effect profile of all EGFR inhibitors, is currently the drug for first-line treatment of EGFR mutant NSCLC, particularly in patients with BM [31]. If not available in the first line, first or second-generation agents should be administered, and in case of progression, efforts should be made to confirm T790 resistance mutation from liquid biopsy or repeated histological sampling. In the presence of a T790 resistance mutation, osimertinib is preferred while platinum-based chemotherapy is recommended in case of negative resistance mutation status. With the widespread use of osimertinib, the development of new resistance mutations is expected. Most commonly, mutation of exon 20 C797X, MET amplification, and HER 2 amplification have been described in addition to aberrations of other non-EGFR mediated pathways [1].
Immunotherapy and targeted treatment options
The IMpower 150 phase 3 three-arm trial compared the combination of chemotherapeutic doublet immunotherapy and VEGF inhibitor with VEGF inhibitor-chemotherapeutic doublet and chemo-immunotherapy. EGFR mutant patients were also eligible for inclusion in the study. Subgroup analyses showed that a significant OS benefit was achieved with the combination of four regimens vs. VEGF inhibitor-chemotherapy doublet, regardless of the presence of EGFR mutations (EGFR positive subgroup mOS 26.1 months vs. 20.3 months; respectively), making the combination of four regimens an additional option after exhaustion of targeted therapies [32].
NSCLC harboring a rare EGFR mutation
Approximately 10%–20% of non-small cell lung tumors carrying EGFR mutations carry rare EGFR mutations [33]. While the presence of classical activating mutations is a strong predictor of favorable tumor response to EGFR tyrosine kinase inhibitors, rare EGFR mutations, such as the exon 20 insertion mutation, are heterogeneous, largely resistant to first- and second-generation drugs, and the efficacy of third-generation osimertinib is limited. In recent years, several new products have been developed for this patient group. Mobocertinib is an irreversible EGFR and HER inhibitor targeting exon 20 alterations. In the phase 1/2 EXCLAIM trial, mobocertinib in the multilineage setting resulted in a 32% tumor response and a median progression-free survival of 7.3 months. Based on the phase 1/2 results, mobocertinib received Food and Drug Administration (FDA) approval. Amivantamab is a bispecific monoclonal antibody that prevents tumor growth and progression by blocking EGFR and c-MET pathways and stimulates immune-mediated destruction of EGFR and cMET-expressing cells. In the CHRYSALIS phase 1 study, patients with exon20 insertion mutations received multiple lines of amivantamab treatment, with an mPFS of 8.3 months and an ORR of 40%. Based on this study, the FDA approved amivantamab for the treatment of patients progressing on platinum-based chemotherapy. Although the use of amivantamab and mobocertinib has improved the tumor response and progression-free survival of this poor prognosis patient group, the presence of EGFR exon 20 insertions is still associated with poor prognosis and unfavorable survival, and further studies on drug development are needed [33].
In addition to the exon 20 insertion mutation, the most common rare mutations include exon 18 G719X, exon 20 S768I, and exon 21 L861Q, often in associated with other mutations [2]. Most clinical trials conducted to date have recruited patients with classical EGFR exon 19 deletion and exon 21 point mutations. An exception was the LUX-lung 2,3,6 trial (afatinib vs. chemotherapy), which included patients with rare EGFR mutations. Following a detailed, retrospective analysis of the trials, the benefit of afatinib in this patient group in terms of tumor response and PFS was published, leading to the registration of afatinib for the treatment of NSCLs with rare EGFR mutations. In the FLAURA 3 study comparing osimertinib and first-generation EGFR TKIs, rare EGFR mutation was an exclusion criterion, but in phase 2 Korean study (KCSG-LU15-09), patients with rare mutations showed a better tumor response and progression-free survival with osimertinib treatment, which was confirmed in some small patient studies. First-generation formulations have shown little activity in rare mutations. Although data are scarce, real-world studies to date suggest the use of second or third-generation drugs, afatinib or osimertinib, in the presence of a major EGFR rare mutation. The choice is a clinical decision, which is best made based on the side effects encountered, the patient’s general condition, and the products’ availability [34].
Summary of EGFR targeted therapy
Treatment recommendation for EGFR mutant metastatic NSCLC based on the ESMO 2023 guideline is shown in Figure 2. In all patients with advanced/metastatic lung tumors, molecular profiling is recommended after histological diagnosis. If an EGFR mutation is confirmed, first-line EGFR tyrosine kinase inhibitor therapy is recommended (I,A). When exon 19 del or exon 21 L858R EGFR mutation confirmed, osimertinib is the first choice, especially in the presence of BM (I, A). As first-line therapy, gefitinib chemotherapy and erlotinib-VEGF inhibitor therapy are also considered (I, B), but due to side effects and higher costs, EGFR TKI therapy alone is the preferred option (I, A). If osimertinib is not available, first-generation (gefitinib, erlotinib) or second-generation (afatnib, dacomitinib) agents are preferred (I, A). In case of progression, liquid biopsy or repeated tissue sampling is recommended to confirm T790 resistance mutation (I, A). In the case of a resistance mutation is present, second-line osimertinib is recommended (I, A), while platinum-based chemotherapy is the treatment of choice in case of negative results (III, A). In the case of osimertinib resistance, next-generation sequencing (NGS) is recommended to detect resistance genes (III, C). Enrolling in a clinical trial is a preferred option if available (III, B) (III, B). Otherwise, platinum-based chemotherapy is administered (III, A). After exhaustion of TKIs, chemotherapy doublet-immunotherapy-VEGF-quadruplet combination may be considered in patients with good overall Eastern Cooperative Oncology Group (ECOG PS) 0–1, if immunotherapy is not contraindicated (III, B) [1]. If oligoprogression is confirmed during EGFR tyrosine kinase inhibitor therapy, local metastasis treatment is recommended, while targeted therapy should be continued (III, A) [1]. In the presence of a rare mutation, non-exon 20 insertion, osimertinib, or afatinib is recommended (III, B). In the presence of exon20 insertion mutations, amivantamab can be given as second-line therapy in the case of progression after first-line therapy (III, B), while mobocertinib EMA approval is pending in these clinical settings (III, C) [1].
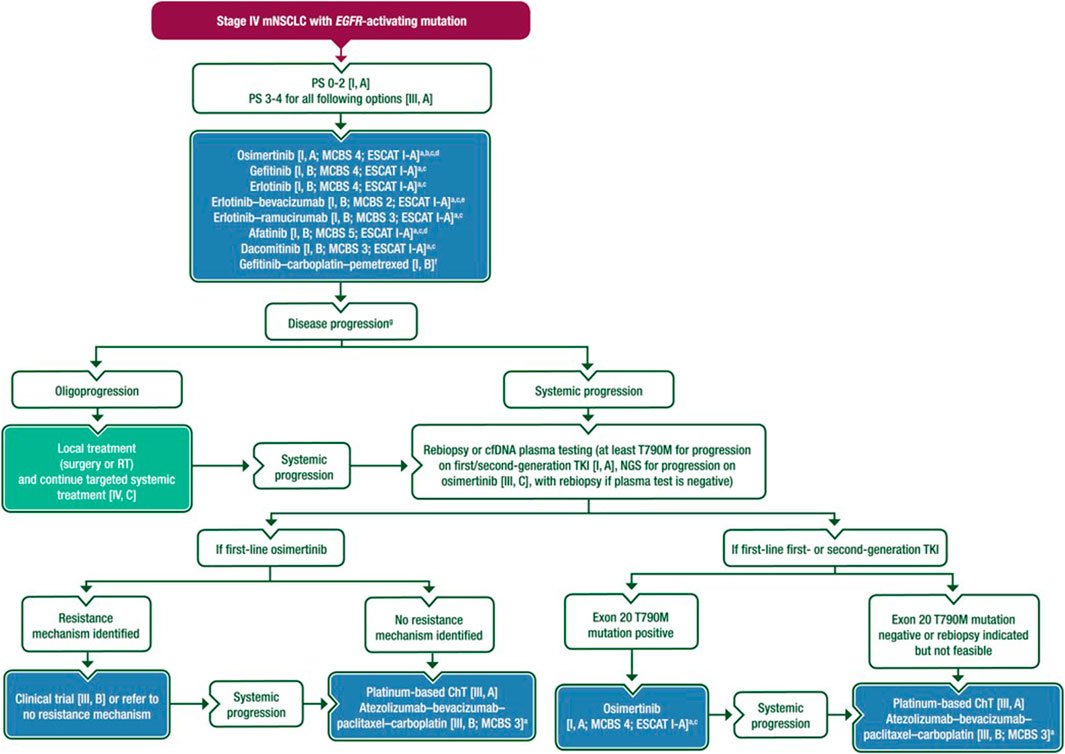
Figure 2. Treatment recommendation for EGFR mutant metastatic NSCLC based on the ESMO 2023 guideline [1].
Treatment of NSCLC with anaplastic lymphoma kinase (ALK) genetical alterations
ALK fusion genes are potent, albeit uncommon, driver oncogenes of non-small cell lung cancer. Notably, the detection of ALK fusion oncogene is of great importance because ALK-positive tumors are highly sensitive to ALK inhibitors, which significantly improves the life expectancy of patients.
Diagnosis
Molecular testing for ALK fusion can be performed as part of standard clinical care in non-small cell lung cancer, primarily adenocarcinoma, from both tumor tissue and plasma samples [35]. Methods for detecting ALK translocation include NGS, IHC, Fluorescence in situ hybridization (FISH), RT-PCR. The standard methodology is FISH, but immunohistochemistry with monoclonal antibodies of high sensitivity and specificity and a validated method is an equivalent method for detecting ALK fusion oncoprotein. RNA-based multigene NGS assays are also suitable instead of IHC or FISH, with the advantage of simultaneous testing for other fusion oncogenes [36, 37].
Epidemiology
The ALK fusion oncogene is present in 3%–5% of non-small cell lung cancers, with the majority of lung cancers carrying the gene being adenocarcinoma (97%). It is a disease of non-smokers or light smokers (<10 pack-years). Relative younger age at onset, with a median age of 52 years. The incidence of ALK molecular alteration in squamous cell carcinoma is limited. Cerebral metastasis is common, approximately 30% at the time of disease discovery [38, 39].
First-line treatment of ALK-positive lung cancer with ALK tyrosine kinase inhibitor (ALK-TKI)
Crizotinib is a multitarget TKI, the first ALK inhibitor to improve the life expectancy of ALK-positive patients compared to chemotherapy in both first-line and subsequent-line settings.
In the phase 3 PROFILE 1014 trial, therapy-naive patients were included, and first-generation ALK inhibitor, crizotinib, was compared with pemetrexed and platinum doublet chemotherapy, and crossover was allowed [40]. At a median follow-up of 17 months, the primary endpoint, progression-free survival, was longer with crizotinib than with chemotherapy (median 10.9 vs. 7 months; HR 0.45, 95% CI 0.35–0.60). Objective tumor response was also increased (74% vs. 45%). At 46 months follow-up, there was no significant difference in overall survival (HR 0.76, 95% CI 0.55–1.05). However, after crossover adjustment, crizotinib also improved overall survival compared with chemotherapy (HR 0.35, 95% CI 0.08–0.72). The median overall survival of more than 4 years was reported in the crizotinib arm [40].
Ceritinib, a second-generation ALK inhibitor, has also been shown to be superior to chemotherapy when administered as first-line therapy [41].
The second-and third-generation ALK inhibitors are more effective than crizotinib in metastatic disease, including BM based on phase 1 randomized controlled trials, and are considered the preferred first-line agents. Second-generation ALK-TKIs are alectinib, brigatinib, and ensartinib (not approved by the European Medicines Agency (EMA)), and third-generation agents are lorlatinib [42–45].
Alectinib indicated for therapy naïve patients in first-line or previously treated with crizotinib in locally advanced or metastatic ALK-positive non-small cell lung cancer. In the phase 3 ALEX randomized controlled trial (N = 303), the median progression-free survival (mPFS) in the first-line setting compared with alectinib plus crizotinib was 35 months for alectinib and 11 months for crizotinib (HR 0.43, 95% CI 0.32–0.58). The results are not yet mature; the median overall survival (mOS) for the alectinib arm was not yet reached, and for the crizotinib arm, it was 57 months (HR 0.67 95% CI 0.46–0.98). Immature data showed a 5-year OS rate of 63% (alectinib) and 46% (crizotinib). Time to CNS progression was longer for alectinib than crizotinib (HR 0.16, 95% CI 0.10–0.28) in the overall population. The rates of grade 3–5 toxicity were similar for alectinib and crizotinib (52% vs. 56%). In the Alectinib arm, there was a higher incidence of anemia, myalgia, se bilirubin elevation, weight gain, and photosensitivity. Nausea, vomiting, and diarrhea were more frequent on the crizotinib arm [42, 46].
Brigatinib is currently approved for use in ALK-positive non-small cell lung cancer in locally advanced or metastatic ALK-positive patients previously treated with crizotinib or not previously treated with an ALK inhibitor. Brigatinib shows efficacy in a broad spectrum of ALK mutations. The phase 3 ALTA-1L randomized controlled trial (N = 275) compared brigatinib with crizotinib in ALK-TKI naive patients. Chemotherapy administration prior to randomization was not an exclusion criterion in the trial. In ALK inhibitor naïve ALK-positive patients at 3-year follow-up, the PFS was 43% vs. 19% for crizotinib vs. crizotinib arm, respectively, according to a standardized independent evaluation. mPFS at 9–11 months follow-up was 24 months versus 11 months (HR 0.48, 95% CI 0.35–0.66). The therapeutic benefit was observed in all subgroups and was prominent in patients with BM. The brain metastasis-related tumor response was significantly higher with brigatinib compared with crizotinib (78% versus 26%). mOS has not yet been reached by either group.
There was ILD/pneumonitis occurred in 4% of patients on brigatinib and 2% on crizotinib. The incidence of grade 3–4 ILD/pneumonitis was 3% versus 0.7%. The risk decreased by gradually increasing the dose of brigatinib (90 mg once daily for 7 days, then increased to 180 mg/day if tolerated). Symptoms associated with elevated creatine kinase (myalgia, muscle pain) did not differ significantly between the two agents. Nausea, diarrhea, constipation, peripheral edema, elevated liver function (GPT), and visual disturbances were more frequent with crizotinib. Grade ≥3 adverse events occurred in 61% with brigatinib and 55% with crizotinib [43].
Lorlatinib is recommended as monotherapy for adult patients with advanced ALK-positive non-small cell lung cancer who have not been previously treated with an ALK inhibitor. It is also for patients with advanced-stage ALK-positive NSCLC whose disease has progressed on first-line treatment with alectinib ceritinib or crizotinib.
In the phase 3 CROWN randomized controlled trial (N = 296), patients with the locally advanced or metastatic stage-naive disease were randomized to the lorlatinib or crizotinib arm. The mPFS was significantly better with lorlatinib than with crizotinib. In the first interim analysis, mPFS at 18 months of follow-up was not yet reached with lorlatinib versus 9.3 months with crizotinib (HR 0.28 95% CI 0.19–0.41). Lorlatinib showed robust CNS efficacy. Grade 3–4 adverse events occurred in 72% of patients treated with lorlatinib and 56% with crizotinib. Hypercholesterolaemia and hypertriglyceridemia occurred in >70% of patients on lorlatinib and neurocognitive side effects may affect the first-line use of lorlatinib [45, 47, 48].
Duration of treatment
Treatment with ALK inhibitors is continued until disease progression. In the case of oligoprogression, local intervention is recommended in addition to the continuation of ALK-TKI. A more potent next-generation ALK inhibitor or standard chemotherapy is indicated for extensive progressive disease.
Treatment for progression on crizotinib
For progression following crizotinib, alectinib or brigatinib is recommended, given their systemic and CNS efficacy and good tolerability.
Alectinib—In the phase 3 ALUR study (N = 107), patients with advanced ALK-positive disease pretreated with platinum-based chemotherapy and crizotinib were randomized to alectinib or mono-chemotherapy (pemetrexed or docetaxel). PFS was longer with alectinib, 7.1 months vs. 1.6 months (HR 0.32, 95% CI 0.17–0.59), and the number of grades ≥3 adverse events was lower with alectinib (27% versus 41%). CNS efficacy was also better with alectinib [49].
Brigatinib—In the phase 2 ALTA study (N = 222), patients refractory to crizotinib at 1 × 90 mg/day (arm A) or 1 × 180 mg/day (arm B) after a seven-day 1 × 90 mg/day lead-in period with brigatinib had an mPFS of 9.2 months versus 16.7 months at lower and higher doses of the agent, respectively. The median overall survival (OS) was 29.5 months versus 34.1 months. In patients with baseline BM, the independently assessed CNS objective tumor response was 50% versus 67%. Both arms had low rates of grade ≥3 toxicity [50].
Ceritinib is not preferable because it is less effective than the former in cross-trial comparisons. In the open-label ASCEND-5 study, 231 patients were randomized to ceritinib 750 mg/day or chemotherapy arm after crizotinib treatment, with ceritinib having better PFS (5.4 versus 1.6 months; HR 0.49) and ORR (39.1% versus 6.9%), both statistically significant. Nevertheless, OS analysis is still immature. Due to crossover, the OS advantage is expected to be decreased in the ceritinib arm. While initial studies used a ceritinib dose of 750 mg/day with fasting intake, a randomized open-label trial found an equivalent dose of 450 mg/day with meals was associated with lower gastrointestinal toxicity [51].
Although a phase 2 trial has shown lorlatinib to be effective in progression on crizotinib (ORR 69%, intracranial ORR 68%, mPFS not yet achieved), the EMA prescribing after crizotinib requires the prior use of a second-generation TKI [48, 52].
Treatment for progression on second-generation ALK TKI
Lorlatinib is a third generation ALK-TKI. Lorlatinib is effective against acquired resistance mutations in most ALK kinase domains, including G1202R and other ALK kinase domain mutations. Lorlatinib is the preferred agent for alectinib-induced resistance [53]. This is probably also true for other second-generation ALK inhibitors [52]. Lorlatinib is also characterized by high CNS penetration.
In a phase 2 trial, lorlatinib in patients previously treated with one or more ALK inhibitors resulted in high objective tumor response (47%), complete remission (2%) and partial tumor response (45%). Following crizotinib, treatments with lorlatinib, the ORR was 73%, and mPFS was 11.1 months. After one or more second-generation ALK inhibitors, ORR was 40% and mPFS was 6.9 months. At >30 months median follow-up, mOS was 21 months. The most common adverse events in this study were hypercholesterolemia (81%), hypertriglyceridemia (61%), edema (43%) and peripheral neuropathy (30%). Serious treatment-related adverse events developed in 7% of patients, the most common being cognitive impairment (1%). In patients who progressed with second generation ALK-TKI, the ORR for lorlatinib was higher when an ALK mutation was present in addition to the ALK fusion oncogene, suggesting that second generation ALK mutations may be associated with the development of a new oncogene. Therefore, genotyping ALK mutations after progression on second generation ALK inhibitors may identify patients more likely to benefit from lorlatinib treatment [52].
Although lorlatinib has not been studied in comparison with chemotherapy in alectinib-resistant disease, lorlatinib after alectinib is recommended because chemotherapy can only achieve poorer survival after progression from ALK-TKI.
Alternative target therapies -ceritinib and brigatinib also show activity in progression after alectinib based on small observational studies [54, 55].
Treatment options for subsequent lines in ALK-positive NSCLC
The IMpower 150 trial suggests chemo-immunotherapy + VEGF inhibitor, the median PFS in patients with EGFR activating mutation + ALK-positive subgroup in TKI pretreated patients were 9.7 vs. 6.1 months; respectively, (HR 0.59, 95% CI 0.37–0.94). Nevertheless, there is no evidence on the efficacy of mono-immunotherapy in the presence of ALK-positivity. Chemotherapy alone is an acceptable additional option with moderate activity in this patient population. Some experts recommend a standard combination of pemetrexed, carboplatin, and pembrolizumab combinations for lung adenocarcinoma, although clinical trials demonstrating the efficacy of this combination have excluded ALK-positive patients [56, 57].
Treatment of brain metastases in ALK-positive NSCLC
In cases of BM, both for symptomatic or asymptomatic cases, second or third generation ALK-TKI is recommended, as these agents have good blood barrier penetration and CNS efficacy. The majority of patients with BM, whether TKI naïve or treated with crizotinib, are likely to respond to these agents and may be able to defer surgical intervention or radiotherapy, thereby reducing morbidity associated with local care. However, surgical treatment may be considered as initial therapy in cases of spatial disproportionation or risk of herniation due to massive BM [58].
Summary of ALK targeted therapy
Treatment recommendation for ALK translocated metastatic NSCLC based on the ESMO 2023 guideline is shown in Figure 3. NSCLC with ALK rearrangements is a subtype of lung cancer with specific clinical and pathological features. Due to the availability of effective therapies, all lung adenocarcinomas should be investigated for ALK fusion oncogenicity. In locally-advanced or metastatic stage ALK-positive NSCLC, a second or third-generation ALK inhibitor is recommended in the frontline setting. Treatment should be continued until progression or intolerable toxicity. In case of oligoprogression in mildly symptomatic or asymptomatic patients, local ablative therapy for the progressive formulation is recommended with continuation of the ALK inhibitor. For progression on a second-generation ALK inhibitor, lorlatinib is recommended over chemotherapy or other ALK inhibitors. Following the exhaustion of TKIs, platinum doublet CHT or in CHT combination with bevacizumab and/or anti-PD immunotherapy can be administered if the patient is still fit for further treatment.
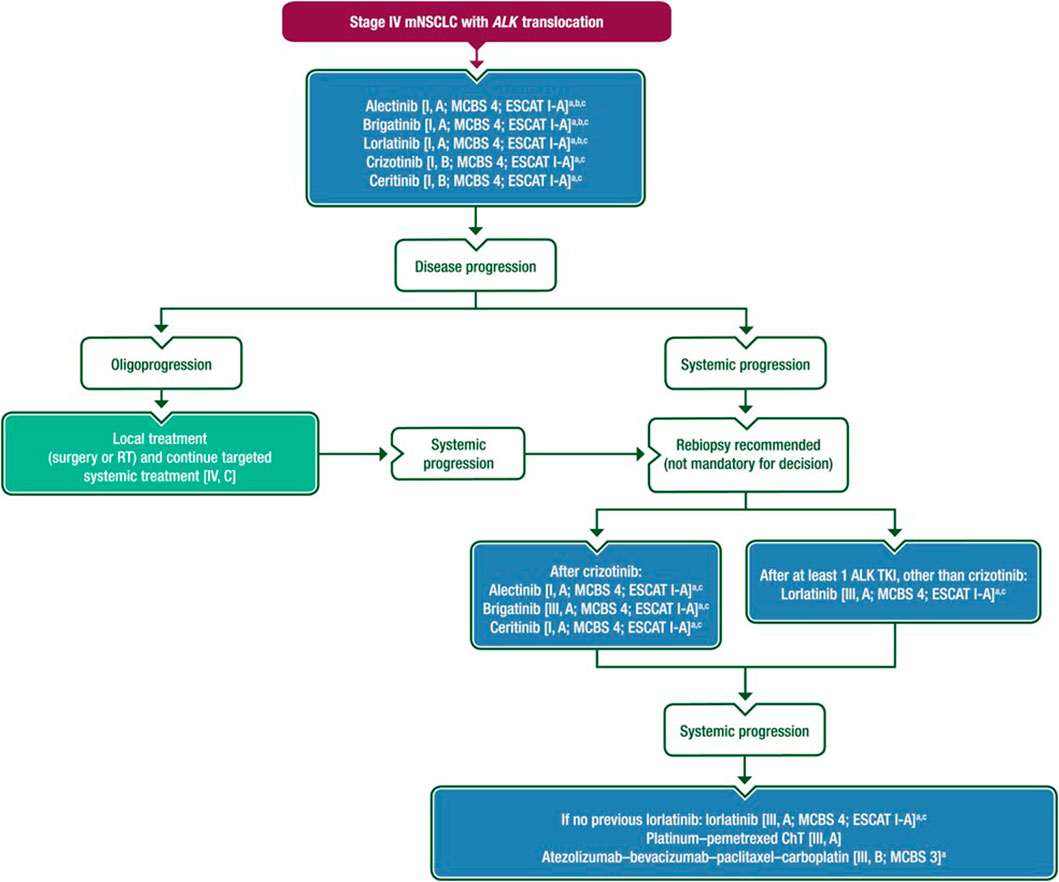
Figure 3. Treatment recommendation for ALK translocated metastatic NSCLC based on the ESMO 2023 guideline [1].
Further studies are needed for TKI-treated ALK-positive cases to determine whether identifying specific tyrosine kinase domain mutation can identify appropriate next steps in therapy. Nevertheless, some preliminary data suggest that specific kinase domain mutations may impact the following line of therapy [2]. Broad genomic profiling may be the most informative approach to examining potential resistance mechanisms, which may require repeated sampling during treatments. Assay methodology selection can impact the ability to identify subclonal events in this setting.
KRAS mutant NSCLC treatment
KRAS mutations activate several additional signaling pathways, occur in about 20%–25% of lung adenocarcinomas and are usually associated with lung cancer in smokers [59]. G12G KRAS mutation subtype is associated with smoking status [6].
The presence of the KRAS mutation in early lung cancer does not seem to affect overall survival, however others have shown that it is associated with a poor prognosis [60]. The focus of targeted therapy for KRAS mutant lung cancer is on irreversible inhibitors of KRAS G12C. KRAS G12C mutations account for nearly 50% of all KRAS mutations [60].
Treatment of non-small cell lung cancer with KRAS G12C mutation
First line treatment
First-line therapy regimens are recommended similarly to non-oncogene-dependent, non-squamous NSCLC [1].
Second-line treatment
Targeted treatment for KRAS G12C mutant tumors after first-line platinum-based chemotherapy and/or anti-PD immunotherapy is considered.
Sotorasib is the first target agent to receive regulatory approval for KRAS G12C mutant locally advanced or metastatic adenocarcinoma in patients who have received at least one prior systemic therapy [61].
In the randomized, open-label, phase 3 CodeBreak 200 trial (N = 345), patients with KRAS G12C mutations were randomized to sotorasib or docetaxel after progression on platinum-based chemotherapy and anti-PD immunotherapy treatment. Better PFS was achieved with sotorasib than docetaxel based on independent unblinded assessment (5.6 versus 4.5 months HR 0.66, 95% CI 0.51–0.86), with fewer grade ≥3 toxicities (33 versus 40%) and fewer serious adverse events (11 versus 23%). Overall survival was similar in the two groups (10.6 months with sotorasib and 11.3 months with docetaxel, HR 1.0). The most common grade ≥3 treatment-related adverse events were diarrhea (12%) and elevated transaminase levels (5%–8%) [62].
In the phase 1 CodeBreak 100 trial, sotorasib achieved an objective tumor response of 41%, mPFS of 6.3 months, OS of 12.5 months, and a two-year survival rate of 33% [63].
Several drug interactions are known to occur with sotorasib. It is not recommended for co-administration with antacids such as proton pump inhibitors, H2 receptor blockers, potent cytochrome P450 3A4 (CYP3A4) inducers, and certain CYP3A4 and P-gp substrates [61].
Adagrasib has been granted conditional marketing authorization by the EMA to treat advanced non-small cell lung cancer with KRAS G12C mutation and progression on at least one prior systemic therapy [64].
In the Krystal-1 single-arm, phase 1–2 study (N = 116), KRAS G12C mutant patients received 2 × 600 mg of adjuvant adagrasib daily after prophylactic chemotherapy and PDL1 inhibitor immunotherapy. The mPFS was 6.5 months, objective tumor response was 43%, the median duration of response was 8.5 months, and OS was 12.6 months. In 33 patients with previously treated stable BM, the intracranial confirmed objective response was 33%. Grade ≥3 treatment-related adverse events occurred in 45% of patients, the most common being fatigue, nausea and elevated liver function tests. Two grade 5 events occurred: heart failure in a patient previously known to have pericardial effusion and one pulmonary hemorrhage [65].
Summary of targeted therapy in KRAS mutant NSCLC
For patients with KRAS G12C mutant NSCLC progressed after a prior line of therapy, second-line sotorasib or adagrasib may be recommended over subsequent chemo and/or immunotherapy.
Treatment of NSCLC with ROS1 genetical alterations
The ROS1 proto-oncogene encodes a tyrosine kinase of the insulin receptor family, which is structurally similar to ALK. ROS1 gene fusion was first identified in 1987 in the glioblastoma cell line U118MG [66]. Since then, ROS1 gene rearrangements have been observed in 22 adult and pediatric malignancies [67]. It is detectable in 1%–2% of NSCLC, with a higher prevalence in non-smoking, younger women. ROS1 mutations do not co-occur with other driver mutations, with rare exceptions including in EGFR (1/166) and KRAS (3/166) and no co-occurring ROS1 and ALK alterations [68]. They are almost exclusively detected in adenocarcinoma, but rare cases are also found in squamous cell, pleiomorphic, and large cell lung carcinoma [69]. FISH is the gold standard method for the detection of ROS1 gene rearrangements. IHC has high sensitivity but low specificity and is not recommended as a primary determinant for treatment. In the case of a positive or inconclusive ROS1 IHC result, confirmatory FISH, NGS, and RT-qPCR should be performed [69, 70]. Treatment recommendation for ROS1 translocated metastatic NSCLC based on the ESMO 2023 guideline is shown in Figure 4.
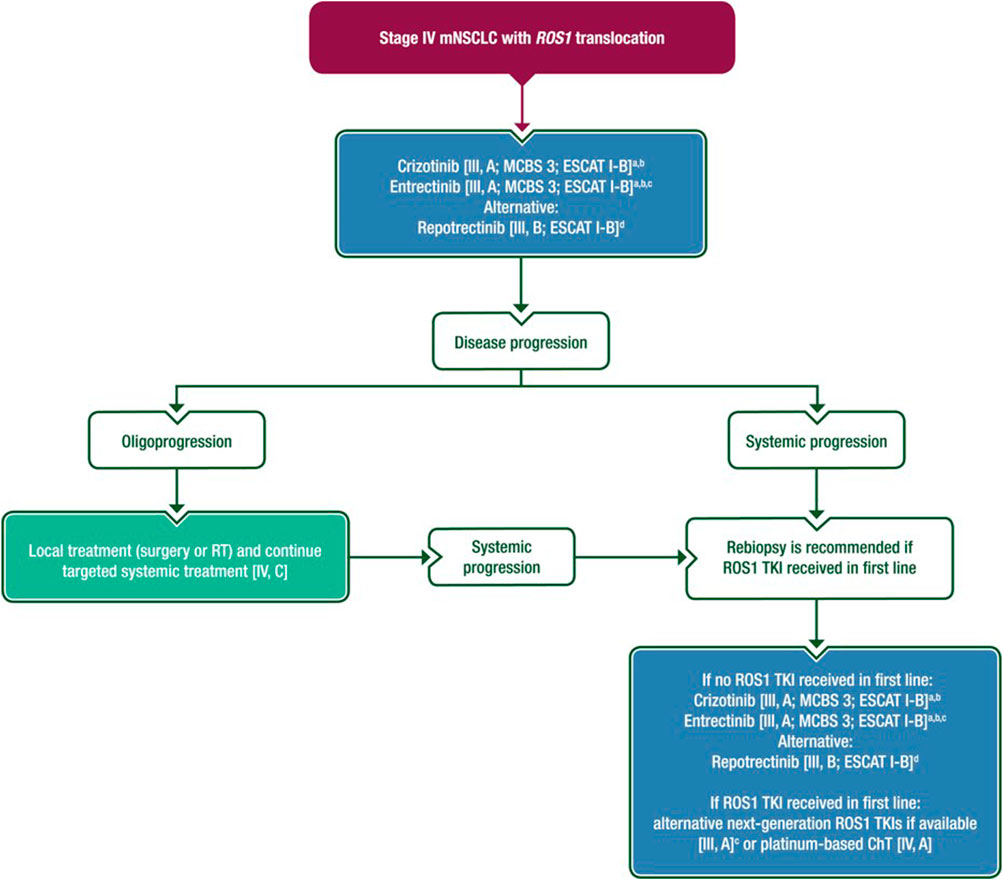
Figure 4. Treatment recommendation for ROS1 translocated metastatic NSCLCbased on the ESMO 2023 guideline [1].
Crizotinib was the first TKI inhibitor to be approved by both the EMA and the FDA for the treatment of ROS1 mutant non-small cell lung cancer based on the results of the phase 1 PROFILE 1001 clinical trial [71]. The study cohort included 53 patients with ROS1-positive NSCLC, most of whom (87%) had previously received first-line platinum-based chemotherapy. The ORR for crizotinib was 72%, associated with a disease control rate (DCR) of 90%. The mPFS and mOS were 19.3 and 51.4 months, respectively. The median duration of therapy with treatment was 22.4 months (15.0–35.9 months) [71]. Subsequently, several retrospective and prospective phase 2 studies have demonstrated the efficacy of crizotinib [69]. However, it is important to emphasize that the drug has a low BBB penetration and, due to the poor brain penetration with crizotinib, the primary site of progression is the central nervous system [72].
Entrectinib is a new generation TKI that inhibits tropomyosin-related kinases in addition to its anti-ROS1 activity. Based on the results of an analysis of data from three prospective phase 1 and 2 clinical trials (ALKA-372–001, STARTRK-1, STARTRK-2), the ORR with entrectinib was 67% and mPFS was 15.7 months. A significant proportion of the 161 patients included in the study (62.7%) had received prior systemic therapy and 34.8% had BM at baseline. The 24 patients who had measurable BM at diagnosis had an intracranial ORR of 79%, mPFS of 12 months and mOS of 26.3 months. The majority of adverse events associated with entrectinib were grade 1 and 2, and overall, the tolerability and safety profile of the agent was similar to other ROS1 inhibitors [73, 74]. Based on these results, entrectinib was granted a marketing authorization by the FDA in 2019 and by the EMA in 2020. Entrectinib is the first line drug for known BM based on the ESMO 2023 recommendation [1].
Ceritinib is a second-generation ALK/ROS1 TKI with significant central nervous system activity. In a phase 2 clinical trial in Korea, 32 patients with advanced ROS1-positive disease, mostly crizotinib-naive (n = 30), were treated with ceritinib. In the whole cohort, ORR was 62%, mPFS was 9.3 months, and DCR was 81%. Among patients who had not received crizotinib treatment, ORR reached 67% and mPFS 18.3 months. Of note, no treatment response was observed in the two patients previously treated with crizotinib while on ceritinib [75]. Based on these results, ceritinib may be considered for crizotinib treatment in patients with ROS1-positive NSCLC who have not previously received crizotinib; however, currently, the agent is neither FDA nor EMA-approved.
Lorlatinib is a third-generation ALK/ROS1 TKI that penetrates the brain and has been effective in a phase 1 and phase 2 single-arm clinical trial that enrolled 69 ROS1-positive patients [52, 76]. The ORR in the TKI-naïve cohort (n = 21) was 62%, mPFS 21 months, and intracranial ORR 64%, compared to a group of previously crizotinib-treated patients (n = 40), where ORR was only 35%, mPFS 8.5 months, and intracranial ORR 50%. There was also a significant difference in the median duration of response (mDOR) (25.3 months vs. 13.8 months). Along with ceritinib, lorlatinib does not have FDA or EMA approval.
Repotrectinib is a new generation ROS1/TRK/ALK tyrosine kinase inhibitor. In the phase 1/2 TRIDENT-1 clinical trial in the ROS1 TKI-naïve group (n = 71), ORR was 79% and mDOR was 34.1 months [77, 78]. In patients who had previously received ROS1 TKI therapy but did not receive chemotherapy/immunotherapy (n = 56), ORR was 38% and mDOR was 14.8 months. Based on these results, in November 2023, the FDA approved repotrectinib to treat ROS1-positive NSCLC [79].
Brigatinib, cabozantinib, thaletrectinib, and ensartinib also have ROS1 inhibitory effects based on preclinical and phase 1/2 studies [80–83].
RET-positive NSCLC treatment
The RET gene encodes a tyrosine kinase-activated membrane receptor protein, primarily involved in the differentiation of the enteric nervous system and urogenital tract [84]. Oncogenic RET alterations can be detected in several solid tumor types [85], such as thyroid cancers, NSCLCs, pancreatic, colorectal, and breast tumors, and are involved in, among others, multiple endocrine neoplasia type 2 [86], and Hirschprung’s disease [87]. RET gene rearrangement is detected in 1%–2% of NSCLCs; these tumors are typically found in non-smoking, younger patients and are associated with an increased risk of BM [88]. Histologically, they are almost exclusively of the adenocarcinoma subtype; others showed 92.3% non-squamous histology [89]. Several fusion partners of RET are known, the most common being KIF5B and CCD6C [90]. IHC and RT-PCR have proven to be unreliable methods for diagnosing RET-positive NSCLCs due to their low sensitivity and variable specificity and are replaced by FISH and NGS [85, 90].
Selpercatinib is a low molecular weight drug that can penetrate the BBB and is a highly selective RET tyrosine kinase inhibitor (TKI) that has demonstrated efficacy in RET translocation-positive NSCLC in the LIBRETTO-001 phase 1/2 clinical trial [91]. The trial enrolled 105 patients previously treated with platinum-based chemotherapy and 39 therapy-naive patients. For pretreated patients, the ORR was 64% (95% CI, 54%–73%) and the mDOR was 17.5 months. In the therapy-naïve group, the ORR was 85% (95% CI, 70%–94%). Of note, 91% of the n = 11 patients with BM observed an intracranial clinical response. The most common grade 3 or more severe adverse events were hypertension (14%), elevated alanine aminotransferase (12%) and aspartate aminotransferase (10%) levels, hyponatremia (6%) and lymphopenia (6%). Based on these results, both FDA (2020) and EMA (2021) have approved selpercatinib for the treatment of locally advanced and metastatic NSCLC [92]. The randomized phase 3 multicentre trial (LIBRETTO-431) compared the efficacy of first-line selpercatinib with or without chemotherapy (carboplatin/cisplatin + pemetrexed) with or without pembrolizumab [93]. The results of the study were presented at the ESMO Congress 2023 [94, 95]. The selpercatinib group had a significantly higher mPFS compared to the chemotherapy ± immunotherapy group (24.8 months vs. 11.2 months; HR:0.465, CI: 0.309–0.699; p < 0.001) [95].
Pralsetinib is the other selective RET inhibitor that will be registered by the FDA in 2020 and by the EMA in 2021, based on the results of the ARROW clinical trial. However, while the EMA approval (for both selprecatinib and pralsetinib) is only valid for patients who have not previously received RET TKI therapy, the FDA approval does not include such a restriction [96–99]. The ORR was 72% in the treatment-naïve (n = 75) and 59% in the group of patients (n = 136) who had received prior platinum-based chemotherapy. The mDOR was not reached in the therapy-naïve group and 22.3 months in the pretreated group. As with selpercatinib, pralsetinib has significant intracranial activity, with an intracranial ORR of 70% (95% CI, 35%–93%) in the group of patients with BM (n = 10, all of whom had received prior chemotherapy) in the study. The agent’s tolerability and side effect profile were similar to the other TKIs [100]. In the ongoing AcceleRET phase 3 clinical trial, similar to the LIBRETTO-431 trial, first-line pralsetinib therapy is being compared with platinum-based chemotherapy ± pembrolizumab [101, 102]. Results of the trial are expected in 2024.
BRAF mutant NSCLC treatment
Mutations in BRAF (V-raf murine sarcoma viral oncogene homolog B) are mutations in the MAPK mitogen-activated protein kinase pathway, which affects downstream signaling proteins. BRAF mutations are alternative oncogenic drivers in NSCLC, which mutually exclude EGFR mutations and ALK and ROS1 rearrangements. The incidence of lung adenocarcinoma is 4.5% [103]. BRAF mutations in the serine/threonine kinase domain most commonly affect V600 [104]. Kinase inhibitors are now available for BRAF V600E mutations. These include dabrafenib, a serine/threonine kinase inhibitor, and trametinib, which has both serine/threonine and tyrosine kinase inhibitory activity [105].
The registration of the drugs was based on a prospective, multicentre, multicohort phase 2 study (BRF113928). The study enrolled 171 patients with metastatic NSCLC with BRAF-V600E mutations, of whom 78 patients received dabrafenib monotherapy (Cohort A), 57 patients received the MEK inhibitor trametinib in combination in multiple lines (Cohort B) and 36 patients received first-line combination therapy (Cohort C). The dose of dabrafenib was 2 × 150 mg/day in both monotherapy and combination therapy, while trametinib treatment was administered at 1 × 2 mg/day. With dabrafenib monotherapy, the response rate (ORR) was 33%, the mPFS was 5.5 months, and the mDOR was 9.6 months. In pretreated patients with the dabrafenib-trametinib combination, the ORR was 68%, mPFS was 10.2 months, and mDOR was 9.8 months. In previously untreated patients on dabrafenib-trametinib combination therapy, the ORR was 64%, mPFS was 10.8 months, and mDOR was 10.2 months. In patients receiving pretreated combination therapy (Cohort B), a median overall survival (OS) of 18.2 months was observed, with 4-year and 5-year survival rates of 34% and 22%, respectively, representing a significant improvement compared to both dabrafenib monotherapy and conventional chemotherapy. The combination of dabrafenib and trametinib is indicated for the treatment of patients with advanced metastatic-stage NSCLC with BRAF V600E mutations (the study on which the registry was based included only BRAF V600 mutation-positive patients, so its efficacy in wild-type BRAF mutant NSCLC has not been proven) [106].
NSCLC with distant metastases should be tested for BRAF V600 mutation status [ESMO II, A]. For NSCLC with BRAF V600E mutation in metastatic stage, first-line treatment with dabrafenib + trametinib is recommended [ESMO III, A; ESCAT: I-B]. If patients have received first-line BRAF and MEK inhibition, platinum-based chemotherapy with or without immunotherapy may be recommended as second-line treatment [ESMO IV, B] [106].
MET exon 14 skipping mutation and MET amplification in NSCLC
Oncogenic activation of the MET (mesenchymal-epithelial transition) signaling pathway can be caused by overexpression, gene amplification, gene rearrangements, and various mutations [1].
MET exon 14 skipping mutations are found in about 3%–4% of younger/smoker/gender patients with NSCLC, mostly in cases where no other driver mutation can be identified, and more often in elderly and smoker patients. In addition to adenocarcinoma, its occurrence has also been observed in sarcomatoid carcinoma. It is considered an unfavorable prognostic marker. The skipping mutation can be detected by DNA- or RNA-based NGS (ESMO IB), while MET amplification can be detected by immunohistochemistry or in situ hybridization (ESMO IIB) [107–109].
Detection of MET overexpression is not associated with effective target therapy, but MET exon 14 skipping mutations or MET amplification is associated with the efficacy of MET inhibitors. MET amplification occurs in 1%–6% of NSCLC cases and may be a cause of acquired resistance to EGFR and ALK inhibitors. For MET amplification, the method of detection and the definition of high gene copy numberstill need to be standardized, while for high gene amplification the MET inhibitor capmatinib has been shown to be effective, but the FDA and EMA have not yet approved its use in this indication. In the case of MET exon 14 skipping mutations, registered targeted treatment options are available. Detection of MET exon 14 skipping mutation and MET amplification is recommended in the initial evaluation of patients diagnosed with non-squamous NSCLC (ESMO IIA).
The FDA has approved capmatinib and tepotinib for the first-line treatment of NSCLC with MET exon 14 skipping mutations, but the EMA has not approved it for first-line, only second- and multiline therapy at present. Thus, first-line platinum-based chemotherapy ± immunotherapy is recommended in these cases.
For patients with MET-amplification, platinum-based chemotherapy with/without immunotherapy is recommended as first-line treatment (ESMO IVB). Following first-line treatment, treatment with capmatinib or tepotinib monotherapy is recommended for patients with MET exon 14 skipping mutation-positive NSCLC (ESMO III A). For tumors carrying less frequent driver mutations, there is little data on the efficacy of immunotherapy, and in these cases, platinum-based chemotherapy or chemotherapy + immunotherapy is recommended if targeted therapy is not an option, while monotherapy immunotherapy is not recommended [108].
Capmatinib
Capmatinib is a potent, selective MET receptor inhibitor and has been shown to be effective in various types of MET activation in vitro and in vivo tumor models [110]. Capmatinib can cross the BBB.
The registration of the medicine was based on the results of the GEOMETRY mono-1 study [110, 111]. The phase 2, open-label, multi-arm study enrolled 364 patients with advanced (stage IIIB or IV) NSCLC who were found to have MET amplification or MET exon 14 skipping mutations. Patients who had received prior chemotherapy and subjects who had not yet received treatment were also included. Patients received capmatinib therapy in the form of 2 × 1,400 mg tablets daily.
In patients with MET exon 14 skipping mutations, the ORR was 41% in previously treated patients and 68% in previously untreated patients. The mPFS was 5.4 months in previously treated subjects and 12.4 months in patients who received first-line treatment. The effect of capmatinib treatment was typically rapid, with the vast majority of patients showing a response (82% of the previously treated patients and 68% of those who had not received treatment previously) having a tumor response at the first tumor evaluation [110]. Of the patients studied, 14 had BM, 12 of whom showed intracranial tumor control, 7 had reduced BM and 4 patients had complete remission.
Among patients, 98% reported some adverse effects, with 67% reporting grade 3–4 adverse effects. The most common symptom was peripheral edema, followed by nausea, vomiting and elevated serum creatinine. The incidence of serious treatment-related adverse events was 13%, with 11% of patients having to stop treatment. Dose reduction was required in 23% of subjects included. In one patient, pneumonitis leading directly to death may likely have been related to capmatinib treatment.
Tepotinib
Tepotinib is also a selective MET tyrosine kinase inhibitor, capable of penetrating the BBB [112]. It has demonstrated efficacy in advanced NSCLC with MET exon 14 skipping mutations in the phase 2 VISION clinical trial [113–115]. Patients with MET amplification were not included in this study. The skipping mutation was detected by histology or liquid biopsy. Patients received the investigational agent in a once-daily oral dose of 500 mg.
In the study, the ORR was 44.7% and the median PFS was 8.9 months. The median overall survival was 17.6 months. Response rates and PFS showed no difference whether the patient received first-line or multi-line treatment with tepotinib. The investigational drug also showed efficacy in elderly patients over 80 (ORR: 35.1%, PFS: 8.6 months). Intracranial tumor control was achieved in the majority of subjects with BM.
Treatment-related adverse events occurred in 86.3% of patients on tepotinib, 24.3% experienced grade 3–4 adverse events, and 12.2% experienced serious adverse events. Three cases were fatal, with death resulting from ILD-related respiratory failure or liver failure. The most common adverse events were peripheral edema, followed by nausea, diarrhea, serum creatinine elevation, and hypoalbuminemia.
HER2 mutant NSCLC treatment
HER2 is a human epidermal growth factor receptor (EGFR/ERBB2) family and is encoded by the ERBB2 gene. The prevalence of HER2 mutations in patients with non-small cell carcinoma is between 1%–4%. HER2 lesions can develop by three mechanisms: HER2 protein overexpression, HER2 amplification and HER2 gene mutation. IHC, FISC and NGS can be used to detect these lesions. Double platinum-based chemotherapy is the first-line treatment of choice and can be complemented with immunotherapy (ESMO IV.B) [116].
In the DESTINY LUNG01 clinical trial, the HER2 antibody-drug conjugate, trastuzumab-deruxtecan treatment efficacy was investigated. In the study, 91 patients with metastatic HER2 mutant NSCLC received second-line trastuzumab-deruxtecan treatment following standard therapy. In the study, PF was 8.2 months (95% CI, 6.0–11.9), while median OS was 17.8 months (95% CI, 13.8–22.1). Treatment-related adverse events included neutropenia and drug-induced ILD, the latter resulting in 2 deaths identified in the study [117].
The DESTINY LUNG02 phase 2 randomized trial also investigated the efficacy and safety of trastuzumab-deruxtecan following platinum-based treatment in the second line, also at two different doses. At both doses (5.4 mg/kg or 6.4 mg/kg every 3 weeks), a significant and sustained antitumor effect with an acceptable safety profile was observed, but the lower dose had a lower rate of drug-induced ILD [118]. The study’s results led to EMA approval of second-line trastuzumab-deruxtecan treatment for NSCLC with metastatic or unresectable HER2 mutations. First line trial phase 3 is recruiting [119].
Treatment of NTRK gene fusion-positive NSCLC
Neurotrophic tyrosine receptor kinase (NTRK) gene fusions initiate downstream signaling pathways, such as the AKT and MEK pathways, and are present at a very low frequency (<1) in solid tumors [1].
Entrectinib is an NTRK and ROS1 inhibitor that can penetrate the central nervous system. In a clinical study of the efficacy of entrectinib in a total of 22 NSCLC patients, the mPFS was 14.9 months (95% Cl, 6.5–30.4), median OS results are not yet available [120].
Larotrectinib is a sensitive tropomyosin receptor kinase inhibitor. In two multicentre clinical trials, a total of 20 NRTK gene fusion-positive patients were tested for the efficacy of larotrectinib. Median PFS outcome was 35.4 months (95% CI, 5.3–35.4), and the median OS was 40.7 months [121].
Discussion
Patients with guideline-recommended molecular alteration-based therapies have better outcomes with first-line targeted therapy for advanced-stage NSCLC [1]. In a retrospective study, others showed a significant increase in OS in patients with non-squamous NSCLC with molecular testing available compared to non-tested patients [122]. Importantly, comprehensive NGS vs. incomplete or no testing before initiating first-line therapy impacts the OS (22.1 vs. 11.6 months, p = 0.017) respectively [123]. Nevertheless, a multidisciplinary approach is essential in finding the proper diagnostic procedures and treatments to personalize NSCLC therapy. There is a broad repertoire of targeted therapies in the standard of care settings. However, there is a need for improvements; therefore, participation in clinical trials is especially encouraged [2]. Accurate imaging-based clinical staging and tissue availability influence subsequent molecular assay-based personalized therapeutic decisions in multidisciplinary teams (MDT) before first line therapy administration. The gold standard for molecular testing in NSCLC is tissue-based testing. Liquid biopsy-based ctDNA detection can guide therapy; however, it should not be used instead of tissue samples. However, the plasma-first approach is recommended if tissue is unavailable [124]. Molecular testing for stage IV NSCLC with reflex testing is associated with shorter turnaround times. There is an emerging requirement for testing in early-stage disease. Formalin-fixed paraffin-embedded (FFPE) material suits for most molecular analyses and non-acid decalcification approaches on bone biopsies. Molecular assays, such as cell blocks, direct smears, or touch preparations, are recommended in order not to miss a targetable genetic alteration. Nevertheless, adequate biopsy sampling should ensure that the sample is suitable for molecular analysis, and in small specimens, minimal IHC should be used to preserve the tissue for molecular studies [2]. Accordingly, the acceptable terms NSCLC favor adenocarcinoma or favor squamous cell carcinoma is recommended with any extent of adenocarcinoma component in a biopsy specimen that is otherwise squamous should trigger molecular testing [2]. At a minimum, EGFR and ALK testing is recommended before initiating immunotherapy because rapid and sensitive tests are available [2, 124]. MDT is best assisted by complete-scale molecular testing for a first-line treatment decision that includes NGS and PDL1 expression [123]. DNA-based NGS oncology panels are recommended to detect EGFR, KRAS, MET, RET, HER2, and BRAF. ALK, ROS1, and NTRK1/2/3 alterations can be identified with FISH. IHC, for screening purposes with low specificity, can also be applied. Therefore, validation with NGS DNA panels with reasonable specificity may detect ALK, RET, and NTRK2 but may underdetect ROS1, NTRK1, and NTRK3 fusions. In the case of RET and METex14, skipping events, RNA-based NGS is preferable to DNA-based NGS or fusion detection [2].
Following the expansion in molecular alteration-based targeted therapy in advanced stages, recently, attention has turned to early-stage cases and resection specimens. Recent advancements in the NSCLC adjuvant treatment setting, the molecular diagnostics for EGFR and ALK in the early stage, indeed necessary to exclude targetable alterations to pave the way to proceed with immunotherapy based on PD-L1 expressors. Accordingly, molecular testing of early-stage resectable NSCLC before neoadjuvant nivolumab plus chemotherapy was performed in CheckMate 816 [125]. Additionally, molecular testing was performed to exclude driver oncogenes in the perioperative early-stage setting in the AEGEAN study on durvalumab plus neoadjuvant chemotherapy [126].
Osimertinib is the first approved targeted therapy based on the ADAURA trial that enrolled patients with classical EGFR mutant (ex19del/L858R) after complete resection, stage I/B -III/A [127, 128]. Adjuvant ALK therapy is currently in a clinical trial [129]. According to an interim analysis of the ALINA trial, adjuvant targeted treatment with alectinib was associated with significant disease-free survival (DFS) benefits compared with platinum-based chemotherapy, with favorable results for alectinib seen in both the stage II–IIIA population (n = 231; hazard ratio [HR] 0.24; 95% confidence interval [CI] 0.13–0.45; p < 0.0001) and the intention-to-treat (ITT) (stage IB–IIIA) population (n = 257; HR 0.24; 95% CI 0.13–0.43; p < 0.0001) [129, 130].
A key factor with targeted therapies includes the control rate of BM; however, there is a significant difference between targeted therapies regarding brain efficacy. New-generation targeted therapies with blood barrier penetration increased the prognosis of brain metastatic NSCLC patients [58]. 20%–30% with advanced NSCLC were found to have BM at diagnosis [131, 132]. Figure 5 shows the distribution of BM according to genetical alterations. A recent meta-analysis suggests that patients with ALK-positive and EGFR-positive NSCLC had higher rates of BM development than other genomic alterations and wild-type tumors [131]. Others showed an association with metastasis development in tumors with ROS1, MET, and RET alterations [131]. However, a meta-analysis does not support a higher rate of BM in these cases compared with wild-type cohorts [131]. BM are frequent in advanced EGFR-mutated or ALK-rearranged NSCLCs, with an estimated >45% of patients with CNS involvement by 3 years of survival with targeted therapies [133].
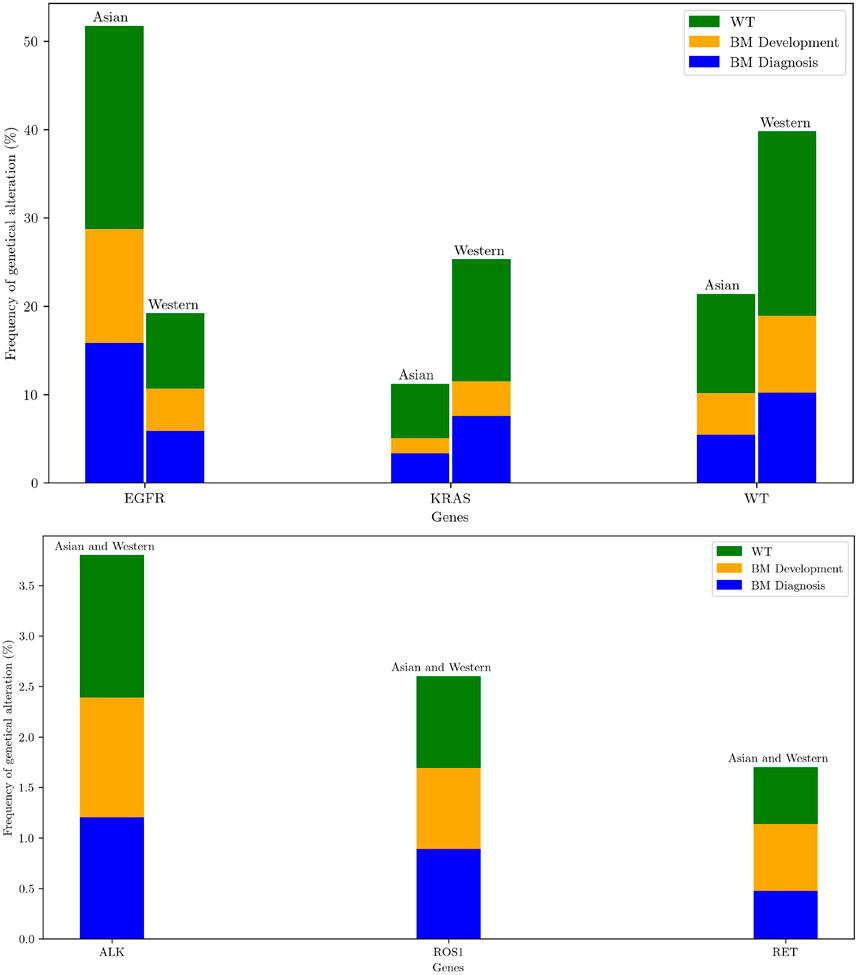
Figure 5. Frequency of oncogenic drivers for East-Asian and Western populations [134]. Bars are stratified according to proportions of brain metastases (BM) at diagnosis (blue) and BM development after diagnosis (orange) and pan-wild-type for all genetic alterations reported including rare ones (WT, green) [131]. For visual enhancement low frequencies of ALK, ROS1, RET genetical alterations are presented in a separate figure.
The intracranial tumor response to TKIs is shown in Table 1 [135]. Patients with EGFR, ALK, and ROS1 positive tumors with oligo- or asymptomatic BM should be treated by upfront systemic targeted therapy [ESMO: III, B] [136]. Of note close MRI surveillance is strongly recommended [1]. The upfront use of radiotherapy might be considered upon BM progression [137]. However, there is no available data on trials comparing the two strategies to assess the impact of delayed radiation in terms of survival or neurologic deficit [138]. ALK inhibitors with CNS activity include Brigatinib, Lorlatinib, and Alectinib [43, 45, 46]. ROS1: Entrectinib is recommended in patients with BM [ ESCAT: I-B]. Compared with earlier-generation drugs, CNS activity of the EGFR TKI, osimertinib showed better intracranial response rates, including stable CNS metastatic cases, in 60% [23, 139].
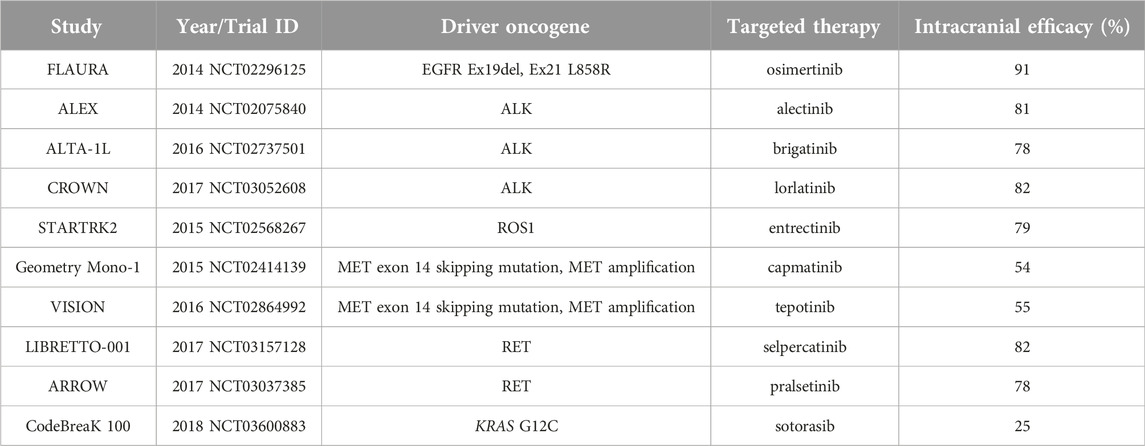
Table 1. Intracranial objective response rate in patients with BM according to the presence of drive oncogenes and targeted therapy administration [135].
Conclusion
Recent expansion in the targeted treatment options into the adjuvant setting of non-small cell lung cancer using accurate pathology diagnostics can minimize the number of excluded patients from molecular diagnostics. Accordingly, careful planning of subsequent hierarchical steps of diagnostic and therapeutic aspects can lead to improved outcomes without excluding patients from best-match targeted therapy. The selection of biopsy procedures and sites, tissue processing, and interpretation, followed by accurate molecular testing-based biomarker identification, is critical. Accordingly, the complexity of theranostics and possible resistance mechanisms can lead to better quality of life and outcomes in special populations, in patients with BM. Future trials should address drug properties such as CNS activity and other special populations, including oligometastatic disease and the emergence of resistance genes to maximize patient survival. Despite the novel standard of care therapies, clinical trials are guideline-recommended options to improve patient outcomes. Accordingly, the therapeutic options are expanding based on the innovative and positive trial results.
Author contributions
GG, ÉM, RK, RH, RB, RP, TL, EG, KY, PK, and ZL: writing, original structure and validation. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Hendriks, LE, Kerr, KM, Menis, J, Mok, TS, Nestle, U, Passaro, A, et al. Oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol (2023) 34:339–57. doi:10.1016/j.annonc.2022.12.009
2. NCCN. NCCN guidelines non-small cell lung cancer version 1 (2024). Available from: https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf (Accessed January 30, 2024).
3. Ahn, M, Arcila, M, Bazhenova, L, Beasley, M, Berezowska, S, Bubendorf, L, et al. IASLC atlas of molecular testing for targeted therapy in lung cancer. Denver: International Association for the Study of Lung Cancer (2023).
4. Fois, SS, Paliogiannis, P, Zinellu, A, Fois, AG, Cossu, A, and Palmieri, G Molecular epidemiology of the main druggable genetic alterations in non-small cell lung cancer. Int J Mol Sci (2021) 22:612. doi:10.3390/ijms22020612
5. Westcott, PMK, Halliwill, KD, To, MD, Rashid, M, Rust, AG, Keane, TM, et al. The mutational landscapes of genetic and chemical models of Kras-driven lung cancer. Nature (2015) 517:489–92. doi:10.1038/nature13898
6. Cserepes, M, Ostoros, G, Lohinai, Z, Raso, E, Barbai, T, Timar, J, et al. Subtype-specific KRAS mutations in advanced lung adenocarcinoma: a retrospective study of patients treated with platinum-based chemotherapy. Eur J Cancer Oxf Engl (2014) 50:1819–28. doi:10.1016/j.ejca.2014.04.001
7. Wu, YL, John, T, Grohe, C, Majem, M, Goldman, JW, Kim, SW, et al. Postoperative chemotherapy use and outcomes from ADAURA: osimertinib as adjuvant therapy for resected EGFR-mutated NSCLC. J Thorac Oncol (2022) 17:423–33. doi:10.1016/j.jtho.2021.10.014
8. Herbst, RS, Wu, Y-L, John, T, Grohe, C, Majem, M, Wang, J, et al. Adjuvant osimertinib for resected EGFR-mutated stage IB-IIIA non-small-cell lung cancer: updated results from the phase III randomized ADAURA trial. J Clin Oncol (2023) 41:1830–40. doi:10.1200/JCO.22.02186
9. Kohno, T, Matsui, T, and Enatsu, S Differences between EGFR exon 19 deletion and exon 21 L858R point mutation, frequently detected EGFR mutations in patients with non-small cell lung cancer, from a molecular biology viewpoint. Gan To Kagaku Ryoho (2021) 48:1463–7.
10. Karachaliou, N, Fernandez-Bruno, M, Bracht, JWP, and Rosell, R EGFR first- and second-generation TKIs—there is still place for them in EGFR-mutant NSCLC patients. Transl Cancer Res (2019) 8:S23–47. doi:10.21037/tcr.2018.10.06
11. Ko, HW, Shie, SS, Wang, CW, Chiu, CT, Wang, CL, Yang, TY, et al. Association of smoking status with non-small cell lung cancer patients harboring uncommon epidermal growth factor receptor mutation. Front Immunol (2022) 13:1011092. doi:10.3389/fimmu.2022.1011092
12. Malapelle, U, Pilotto, S, Passiglia, F, Pepe, F, Pisapia, P, Righi, L, et al. Dealing with NSCLC EGFR mutation testing and treatment: a comprehensive review with an Italian real-world perspective. Crit Rev Oncol Hematol (2021) 160:103300. doi:10.1016/j.critrevonc.2021.103300
13. Fukuoka, M, Wu, Y-L, Thongprasert, S, Sunpaweravong, P, Leong, S-S, Sriuranpong, V, et al. Biomarker analyses and final overall survival results from a phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer in Asia (IPASS). J Clin Oncol (2011) 29:2866–74. doi:10.1200/JCO.2010.33.4235
14. Zhou, C, Wu, YL, Chen, G, Feng, J, Liu, XQ, Wang, C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol (2011) 12:735–42. doi:10.1016/S1470-2045(11)70184-X
15. Rosell, R, Carcereny, E, Gervais, R, Vergnenegre, A, Massuti, B, Felip, E, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol (2012) 13:239–46. doi:10.1016/S1470-2045(11)70393-X
16. Zhou, C, Wu, Y-L, Chen, G, Feng, J, Liu, X, Wang, C, et al. Efficacy results from the randomised phase III OPTIMAL (CTONG 0802) study comparing first-line erlotinib versus carboplatin (CBDCA) plus gemcitabine (GEM) in Chinese advanced non small cell lung cancer (NSCLC) patients (PTS) with EGFR activating mutations. Ann Oncol (2010) 21(supp.8):LBA13. doi:10.1093/annonc/mdq601
17. Chen, KL, Lin, CC, Cho, YT, Yang, CW, Sheen, YS, Tsai, HE, et al. Comparison of skin toxic effects associated with gefitinib, erlotinib, or afatinib treatment for non-small cell lung cancer. JAMA Dermatol (2016) 152:340–2. doi:10.1001/jamadermatol.2015.4448
18. Cárdenas-Fernández, D, Soberanis Pina, P, Turcott, JG, Chávez-Tapia, N, Conde-Flores, E, Cardona, AF, et al. Management of diarrhea induced by EGFR-TKIs in advanced lung adenocarcinoma. Ther Adv Med Oncol (2023) 15:17588359231192396. doi:10.1177/17588359231192396
19. Nakagawa, K, Garon, EB, Seto, T, Nishio, M, Ponce Aix, S, Paz-Ares, L, et al. Ramucirumab plus erlotinib in patients with untreated, EGFR-mutated, advanced non-small-cell lung cancer (RELAY): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol (2019) 20:1655–69. doi:10.1016/S1470-2045(19)30634-5
20. Sequist, LV, Yang, JC-H, Yamamoto, N, O’Byrne, K, Hirsh, V, Mok, T, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol (2013) 31:3327–34. doi:10.1200/JCO.2012.44.2806
21. Wu, Y-L, Zhou, C, Hu, C-P, Feng, J, Lu, S, Huang, Y, et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised phase 3 trial. Lancet Oncol (2014) 15:213–22. doi:10.1016/S1470-2045(13)70604-1
22. Yang, JC-H, Wu, Y-L, Schuler, M, Sebastian, M, Popat, S, Yamamoto, N, et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): analysis of overall survival data from two randomised, phase 3 trials. Lancet Oncol (2015) 16:141–51. doi:10.1016/S1470-2045(14)71173-8
23. Park, K, Tan, E-H, O’Byrne, K, Zhang, L, Boyer, M, Mok, T, et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): a phase 2B, open-label, randomised controlled trial. Lancet Oncol (2016) 17:577–89. doi:10.1016/S1470-2045(16)30033-X
24. Wu, Y-L, Cheng, Y, Zhou, X, Lee, KH, Nakagawa, K, Niho, S, et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, phase 3 trial. Lancet Oncol (2017) 18:1454–66. doi:10.1016/S1470-2045(17)30608-3
25. Mok, TS, Cheng, Y, Zhou, X, Lee, KH, Nakagawa, K, Niho, S, et al. Improvement in overall survival in a randomized study that compared dacomitinib with gefitinib in patients with advanced non-small-cell lung cancer and EGFR-activating mutations. J Clin Oncol (2018) 36:2244–50. doi:10.1200/JCO.2018.78.7994
26. He, J, Huang, Z, Han, L, Gong, Y, and Xie, C Mechanisms and management of 3rd-generation EGFR-TKI resistance in advanced non-small cell lung cancer (Review). Int J Oncol (2021) 59:90. doi:10.3892/ijo.2021.5270
27. Papadimitrakopoulou, VA, Mok, TS, Han, J-Y, Ahn, M-J, Delmonte, A, Ramalingam, SS, et al. Osimertinib versus platinum-pemetrexed for patients with EGFR T790M advanced NSCLC and progression on a prior EGFR-tyrosine kinase inhibitor: AURA3 overall survival analysis. Ann Oncol (2020) 31:1536–44. doi:10.1016/j.annonc.2020.08.2100
28. Ramalingam, SS, Vansteenkiste, J, Planchard, D, Cho, BC, Gray, JE, Ohe, Y, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med (2020) 382:41–50. doi:10.1056/NEJMoa1913662
29. Belani, N, Liang, K, Fradley, M, Judd, J, and Borghaei, H How to treat EGFR-mutated non–small cell lung cancer. JACC CardioOncology (2023) 5:542–5. doi:10.1016/j.jaccao.2023.04.005
30. Vaid, AK, Gupta, A, and Momi, G Overall survival in stage IV EGFR mutation-positive NSCLC: comparing first-second- and third-generation EGFR-TKIs (Review). Int J Oncol (2021) 58:171–84. doi:10.3892/ijo.2021.5168
31. Tatineni, V, O’Shea, PJ, Ozair, A, Khosla, AA, Saxena, S, Rauf, Y, et al. First-versus third-generation EGFR tyrosine kinase inhibitors in EGFR-mutated non-small cell lung cancer patients with brain metastases. Cancers (2023) 15:2382. doi:10.3390/cancers15082382
32. Nogami, N, Barlesi, F, Socinski, MA, Reck, M, Thomas, CA, Cappuzzo, F, et al. IMpower150 final exploratory analyses for atezolizumab plus bevacizumab and chemotherapy in key NSCLC patient subgroups with EGFR mutations or metastases in the liver or brain. J Thorac Oncol (2022) 17:309–23. doi:10.1016/j.jtho.2021.09.014
33. Bai, Q, Wang, J, and Zhou, X EGFR exon20 insertion mutations in non-small cell lung cancer: clinical implications and recent advances in targeted therapies. Cancer Treat Rev (2023) 120:102605. doi:10.1016/j.ctrv.2023.102605
34. Passaro, A, Mok, T, Peters, S, Popat, S, Ahn, M-J, and de Marinis, F Recent advances on the role of EGFR tyrosine kinase inhibitors in the management of NSCLC with uncommon, non exon 20 insertions, EGFR mutations. J Thorac Oncol (2021) 16:764–73. doi:10.1016/j.jtho.2020.12.002
35. Zugazagoitia, J, Ramos, I, Trigo, JM, Palka, M, Gómez-Rueda, A, Jantus-Lewintre, E, et al. Clinical utility of plasma-based digital next-generation sequencing in patients with advance-stage lung adenocarcinomas with insufficient tumor samples for tissue genotyping. Ann Oncol (2019) 30:290–6. doi:10.1093/annonc/mdy512
36. Weickhardt, AJ, Aisner, DL, Franklin, WA, Varella-Garcia, M, Doebele, RC, and Camidge, DR Diagnostic assays for identification of anaplastic lymphoma kinase-positive non-small cell lung cancer. Cancer (2013) 119:1467–77. doi:10.1002/cncr.27913
37. Li, W, Zhang, J, Guo, L, Chuai, S, Shan, L, and Ying, J Combinational analysis of FISH and immunohistochemistry reveals rare genomic events in ALK fusion patterns in NSCLC that responds to crizotinib treatment. J Thorac Oncol (2017) 12:94–101. doi:10.1016/j.jtho.2016.08.145
38. Shaw, AT, Yeap, BY, Mino-Kenudson, M, Digumarthy, SR, Costa, DB, Heist, RS, et al. Clinical features and outcome of patients with non-small-cell lung cancer who harbor EML4-ALK. J Clin Oncol (2009) 27:4247–53. doi:10.1200/JCO.2009.22.6993
39. National Institutes of Health. Cancer of the lung and bronchus - cancer stat facts (2024). Available from: https://seer.cancer.gov/statfacts/html/lungb.html (Accessed January 24, 2024).
40. Solomon, BJ, Mok, T, Kim, D-W, Wu, Y-L, Nakagawa, K, Mekhail, T, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med (2014) 371:2167–77. doi:10.1056/NEJMoa1408440
41. Soria, J-C, Tan, DSW, Chiari, R, Wu, Y-L, Paz-Ares, L, Wolf, J, et al. First-line ceritinib versus platinum-based chemotherapy in advanced ALK-rearranged non-small-cell lung cancer (ASCEND-4): a randomised, open-label, phase 3 study. Lancet Lond Engl (2017) 389:917–29. doi:10.1016/S0140-6736(17)30123-X
42. Camidge, DR, Dziadziuszko, R, Peters, S, Mok, T, Noe, J, Nowicka, M, et al. Updated efficacy and safety data and impact of the EML4-ALK fusion variant on the efficacy of alectinib in untreated ALK-positive advanced non-small cell lung cancer in the global phase III ALEX study. J Thorac Oncol (2019) 14:1233–43. doi:10.1016/j.jtho.2019.03.007
43. Camidge, DR, Kim, HR, Ahn, M-J, Yang, JCH, Han, J-Y, Hochmair, MJ, et al. Brigatinib versus crizotinib in ALK inhibitor-naive advanced ALK-positive NSCLC: final results of phase 3 ALTA-1L trial. J Thorac Oncol (2021) 16:2091–108. doi:10.1016/j.jtho.2021.07.035
44. Horn, L, Wang, Z, Wu, G, Poddubskaya, E, Mok, T, Reck, M, et al. Ensartinib vs crizotinib for patients with anaplastic lymphoma kinase-positive non-small cell lung cancer: a randomized clinical trial. JAMA Oncol (2021) 7:1617–25. doi:10.1001/jamaoncol.2021.3523
45. Shaw, AT, Bauer, TM, de Marinis, F, Felip, E, Goto, Y, Liu, G, et al. First-line lorlatinib or crizotinib in advanced ALK-positive lung cancer. N Engl J Med (2020) 383:2018–29. doi:10.1056/NEJMoa2027187
46. Mok, T, Camidge, DR, Gadgeel, SM, Rosell, R, Dziadziuszko, R, Kim, D-W, et al. Updated overall survival and final progression-free survival data for patients with treatment-naive advanced ALK-positive non-small-cell lung cancer in the ALEX study. Ann Oncol (2020) 31:1056–64. doi:10.1016/j.annonc.2020.04.478
47. Solomon, BJ, Bauer, TM, Ignatius Ou, S-H, Liu, G, Hayashi, H, Bearz, A, et al. Post hoc analysis of lorlatinib intracranial efficacy and safety in patients with ALK-positive advanced non-small-cell lung cancer from the phase III CROWN study. J Clin Oncol (2022) 40:3593–602. doi:10.1200/JCO.21.02278
48. EMA. Summary of the risk management plan for Lorviqua (lorlatinib) (2024). Available from: https://www.ema.europa.eu/en/documents/rmp-summary/lorviqua-epar-risk-management-plan-summary_en.pdf (Accessed January 31, 2024).
49. Novello, S, Mazières, J, Oh, I-J, de Castro, J, Migliorino, MR, Helland, Å, et al. Alectinib versus chemotherapy in crizotinib-pretreated anaplastic lymphoma kinase (ALK)-positive non-small-cell lung cancer: results from the phase III ALUR study. Ann Oncol (2018) 29:1409–16. doi:10.1093/annonc/mdy121
50. Huber, RM, Hansen, KH, Paz-Ares Rodríguez, L, West, HL, Reckamp, KL, Leighl, NB, et al. Brigatinib in crizotinib-refractory ALK+ NSCLC: 2-year follow-up on systemic and intracranial outcomes in the phase 2 ALTA trial. J Thorac Oncol (2020) 15:404–15. doi:10.1016/j.jtho.2019.11.004
51. Shaw, AT, Kim, TM, Crinò, L, Gridelli, C, Kiura, K, Liu, G, et al. Ceritinib versus chemotherapy in patients with ALK-rearranged non-small-cell lung cancer previously given chemotherapy and crizotinib (ASCEND-5): a randomised, controlled, open-label, phase 3 trial. Lancet Oncol (2017) 18:874–86. doi:10.1016/S1470-2045(17)30339-X
52. Solomon, BJ, Besse, B, Bauer, TM, Felip, E, Soo, RA, Camidge, DR, et al. Lorlatinib in patients with ALK-positive non-small-cell lung cancer: results from a global phase 2 study. Lancet Oncol (2018) 19:1654–67. doi:10.1016/S1470-2045(18)30649-1
53. Shaw, AT, Solomon, BJ, Besse, B, Bauer, TM, Lin, CC, Soo, RA, et al. ALK resistance mutations and efficacy of lorlatinib in advanced anaplastic lymphoma kinase-positive non-small-cell lung cancer. J Clin Oncol (2019) 37:1370–9. doi:10.1200/JCO.18.02236
54. Lin, JJ, Zhu, VW, Schoenfeld, AJ, Yeap, BY, Saxena, A, Ferris, LA, et al. Brigatinib in patients with alectinib-refractory ALK-positive NSCLC. J Thorac Oncol (2018) 13:1530–8. doi:10.1016/j.jtho.2018.06.005
55. Yoshida, H, Kim, YH, Ozasa, H, Sakamori, Y, Tsuji, T, Nomizo, T, et al. Efficacy of ceritinib after alectinib for ALK-positive non-small cell lung cancer. Vivo (2018) 32:1587–90. doi:10.21873/invivo.11418
56. Lin, JJ, Schoenfeld, AJ, Zhu, VW, Yeap, BY, Chin, E, Rooney, M, et al. Efficacy of platinum/pemetrexed combination chemotherapy in ALK-positive NSCLC refractory to second-generation ALK inhibitors. J Thorac Oncol (2020) 15:258–65. doi:10.1016/j.jtho.2019.10.014
57. Socinski, MA, Jotte, RM, Cappuzzo, F, Orlandi, FJ, Stroyakovskiy, D, Nogami, N, et al. Overall survival (OS) analysis of IMpower150, a randomized Ph 3 study of atezolizumab (atezo) + chemotherapy (chemo) ± bevacizumab (bev) vs chemo + bev in 1L nonsquamous (NSQ) NSCLC. J Clin Oncol (2018) 36:9002. doi:10.1200/JCO.2018.36.15_suppl.9002
58. Singh, K, Saxena, S, Khosla, AA, McDermott, MW, Kotecha, RR, and Ahluwalia, MS Update on the management of brain metastasis. Neurotherapeutics (2022) 19:1772–81. doi:10.1007/s13311-022-01312-w
59. Moldvay, J, and Tímár, J KRASG12C mutant lung adenocarcinoma: unique biology, novel therapies and new challenges. Pathol Oncol Res (2024) 29:1611580. doi:10.3389/pore.2023.1611580
60. Shepherd, FA, Domerg, C, Hainaut, P, Jänne, PA, Pignon, J-P, Graziano, S, et al. Pooled analysis of the prognostic and predictive effects of KRAS mutation status and KRAS mutation subtype in early-stage resected non-small-cell lung cancer in four trials of adjuvant chemotherapy. J Clin Oncol (2013) 31:2173–81. doi:10.1200/JCO.2012.48.1390
61. Nakajima, EC, Drezner, N, Li, X, Mishra-Kalyani, PS, Liu, Y, Zhao, H, et al. FDA approval summary: sotorasib for KRAS G12C-Mutated metastatic NSCLC. Clin Cancer Res (2022) 28(8):1482–1486. doi:10.1158/1078-0432.CCR-21-3074
62. de Langen, AJ, Johnson, ML, Mazieres, J, Dingemans, A-MC, Mountzios, G, Pless, M, et al. Sotorasib versus docetaxel for previously treated non-small-cell lung cancer with KRASG12C mutation: a randomised, open-label, phase 3 trial. Lancet Lond Engl (2023) 401:733–46. doi:10.1016/S0140-6736(23)00221-0
63. Dy, GK, Govindan, R, Velcheti, V, Falchook, GS, Italiano, A, Wolf, J, et al. Long-term outcomes and molecular correlates of sotorasib efficacy in patients with pretreated KRAS G12C-mutated non-small-cell lung cancer: 2-year analysis of CodeBreaK 100. J Clin Oncol (2023) 41:3311–7. doi:10.1200/JCO.22.02524
64. ESMO. EMA recommends granting a conditional marketing authorisation for adagrasib following a Re-examination procedure (2023). Available from: https://www.esmo.org/oncology-news/ema-recommends-granting-a-conditional-marketing-authorisation-for-adagrasib-following-a-re-examination-procedure (Accessed January 24, 2024).
65. Jänne, PA, Riely, GJ, Gadgeel, SM, Heist, RS, Ou, S-HI, Pacheco, JM, et al. Adagrasib in non-small-cell lung cancer harboring a KRASG12C mutation. N Engl J Med (2022) 387:120–31. doi:10.1056/NEJMoa2204619
66. Birchmeier, C, Sharma, S, and Wigler, M Expression and rearrangement of the ROS1 gene in human glioblastoma cells. Proc Natl Acad Sci U S A (1987) 84:9270–4. doi:10.1073/pnas.84.24.9270
67. Drilon, A, Jenkins, C, Iyer, S, Schoenfeld, A, Keddy, C, and Davare, MA ROS1-dependent cancers - biology, diagnostics and therapeutics. Nat Rev Clin Oncol (2021) 18:35–55. doi:10.1038/s41571-020-0408-9
68. Lin, JJ, Ritterhouse, LL, Ali, SM, Bailey, M, Schrock, AB, Gainor, JF, et al. ROS1 fusions rarely overlap with other oncogenic drivers in non-small cell lung cancer. J Thorac Oncol (2017) 12:872–7. doi:10.1016/j.jtho.2017.01.004
69. Gendarme, S, Bylicki, O, Chouaid, C, and Guisier, F ROS-1 fusions in non-small-cell lung cancer: evidence to date. Curr Oncol Tor Ont (2022) 29:641–58. doi:10.3390/curroncol29020057
70. Lindeman, NI, Cagle, PT, Aisner, DL, Arcila, ME, Beasley, MB, Bernicker, EH, et al. Updated molecular testing guideline for the selection of lung cancer patients for treatment with targeted tyrosine kinase inhibitors: guideline from the college of American pathologists, the international association for the study of lung cancer, and the association for molecular pathology. Arch Pathol Lab Med (2018) 142:321–46. doi:10.5858/arpa.2017-0388-CP
71. Shaw, AT, Riely, GJ, Bang, YJ, Kim, DW, Camidge, DR, Solomon, BJ, et al. Crizotinib in ROS1-rearranged advanced non-small-cell lung cancer (NSCLC): updated results, including overall survival, from PROFILE 1001. Ann Oncol (2019) 30:1121–6. doi:10.1093/annonc/mdz131
72. Fischer, H, Ullah, M, de la Cruz, CC, Hunsaker, T, Senn, C, Wirz, T, et al. Entrectinib, a TRK/ROS1 inhibitor with anti-CNS tumor activity: differentiation from other inhibitors in its class due to weak interaction with P-glycoprotein. Neuro-Oncol (2020) 22:819–29. doi:10.1093/neuonc/noaa052
73. Drilon, A, Siena, S, Dziadziuszko, R, Barlesi, F, Krebs, MG, Shaw, AT, et al. Entrectinib in ROS1 fusion-positive non-small-cell lung cancer: integrated analysis of three phase 1-2 trials. Lancet Oncol (2020) 21:261–70. doi:10.1016/S1470-2045(19)30690-4
74. Dziadziuszko, R, Krebs, MG, De Braud, F, Siena, S, Drilon, A, Doebele, RC, et al. Updated integrated analysis of the efficacy and safety of entrectinib in locally advanced or metastatic ROS1 fusion-positive non-small-cell lung cancer. J Clin Oncol (2021) 39:1253–63. doi:10.1200/JCO.20.03025
75. Lim, SM, Kim, HR, Lee, J-S, Lee, KH, Lee, Y-G, Min, YJ, et al. Open-label, multicenter, phase II study of ceritinib in patients with non-small-cell lung cancer harboring ROS1 rearrangement. J Clin Oncol (2017) 35:2613–8. doi:10.1200/JCO.2016.71.3701
76. Shaw, AT, Solomon, BJ, Chiari, R, Riely, GJ, Besse, B, Soo, RA, et al. Lorlatinib in advanced ROS1-positive non-small-cell lung cancer: a multicentre, open-label, single-arm, phase 1-2 trial. Lancet Oncol (2019) 20:1691–701. doi:10.1016/S1470-2045(19)30655-2
77. Lin, JJ, Drilon, AE, Cho, BC, Felip, E, De Langen, A, Yang, N, et al. Intracranial and systemic efficacy of repotrectinib in advanced ROS1 fusion-positive (ROS1+) non-small cell lung cancer (NSCLC) and central nervous system metastases (CNS mets) in the phase 1/2 TRIDENT-1. J Clin Oncol (2023) 41:9017. doi:10.1200/JCO.2023.41.16_suppl.9017
78. Yun, MR, Kim, DH, Kim, SY, Joo, HS, Lee, YW, Choi, HM, et al. Repotrectinib exhibits potent antitumor activity in treatment-naïve and solvent-front-mutant ROS1-rearranged non-small cell lung cancer. Clin Cancer Res (2020) 26:3287–95. doi:10.1158/1078-0432.CCR-19-2777
79. FDA. FDA approves repotrectinib for ROS1-positive non-small cell lung cancer (2023). Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-repotrectinib-ros1-positive-non-small-cell-lung-cancer (Accessed January 24, 2024).
80. Dudnik, E, Agbarya, A, Grinberg, R, Cyjon, A, Bar, J, Moskovitz, M, et al. Clinical activity of brigatinib in ROS1-rearranged non-small cell lung cancer. Clin Transl Oncol (2020) 22:2303–11. doi:10.1007/s12094-020-02376-w
81. Katayama, R, Gong, B, Togashi, N, Miyamoto, M, Kiga, M, Iwasaki, S, et al. The new-generation selective ROS1/NTRK inhibitor DS-6051b overcomes crizotinib resistant ROS1-G2032R mutation in preclinical models. Nat Commun (2019) 10:3604. doi:10.1038/s41467-019-11496-z
82. Papadopoulos, KP, Borazanci, E, Shaw, AT, Katayama, R, Shimizu, Y, Zhu, VW, et al. U.S. Phase I first-in-human study of taletrectinib (DS-6051b/AB-106), a ROS1/TRK inhibitor, in patients with advanced solid tumors. Clin Cancer Res (2020) 26:4785–94. doi:10.1158/1078-0432.CCR-20-1630
83. Ai, X, Wang, Q, Cheng, Y, Liu, X, Cao, L, Chen, J, et al. Safety but limited efficacy of ensartinib in ROS1-positive NSCLC: a single-arm, multicenter phase 2 study. J Thorac Oncol (2021) 16:1959–63. doi:10.1016/j.jtho.2021.06.023
84. Mulligan, LM RET revisited: expanding the oncogenic portfolio. Nat Rev Cancer (2014) 14:173–86. doi:10.1038/nrc3680
85. Ferrara, R, Auger, N, Auclin, E, and Besse, B Clinical and translational implications of RET rearrangements in non-small cell lung cancer. J Thorac Oncol (2018) 13:27–45. doi:10.1016/j.jtho.2017.10.021
86. Mulligan, LM, Kwok, JB, Healey, CS, Elsdon, MJ, Eng, C, Gardner, E, et al. Germ-line mutations of the RET proto-oncogene in multiple endocrine neoplasia type 2A. Nature (1993) 363:458–60. doi:10.1038/363458a0
87. Romeo, G, Ronchetto, P, Luo, Y, Barone, V, Seri, M, Ceccherini, I, et al. Point mutations affecting the tyrosine kinase domain of the RET proto-oncogene in Hirschsprung’s disease. Nature (1994) 367:377–8. doi:10.1038/367377a0
88. Drilon, A, Lin, JJ, Filleron, T, Ni, A, Milia, J, Bergagnini, I, et al. Frequency of brain metastases and multikinase inhibitor outcomes in patients with RET-rearranged lung cancers. J Thorac Oncol (2018) 13:1595–601. doi:10.1016/j.jtho.2018.07.004
89. Feng, J, Li, Y, Wei, B, Guo, L, Li, W, Xia, Q, et al. Clinicopathologic characteristics and diagnostic methods of RET rearrangement in Chinese non-small cell lung cancer patients. Transl Lung Cancer Res (2022) 11:617–31. doi:10.21037/tlcr-22-202
90. Andrini, E, Mosca, M, Galvani, L, Sperandi, F, Ricciuti, B, Metro, G, et al. Non-small-cell lung cancer: how to manage RET-positive disease. Drugs Context (2022) 11:1–12. doi:10.7573/dic.2022-1-5
91. Drilon, A, Oxnard, GR, Tan, DSW, Loong, HHF, Johnson, M, Gainor, J, et al. Efficacy of selpercatinib in RET fusion-positive non-small-cell lung cancer. N Engl J Med (2020) 383:813–24. doi:10.1056/NEJMoa2005653
92. Duke, ES, Bradford, D, Marcovitz, M, Amatya, AK, Mishra-Kalyani, PS, Nguyen, E, et al. FDA approval summary: selpercatinib for the treatment of advanced RET fusion-positive solid tumors. Clin Cancer Res (2023) 29:3573–8. doi:10.1158/1078-0432.CCR-23-0459
93. Solomon, BJ, Zhou, CC, Drilon, A, Park, K, Wolf, J, Elamin, Y, et al. Phase III study of selpercatinib versus chemotherapy ± pembrolizumab in untreated RET positive non-small-cell lung cancer. Future Oncol Lond Engl (2021) 17:763–73. doi:10.2217/fon-2020-0935
94. Loong, HHF, Goto, K, Solomon, BJ, Park, K, Pérol, M, Arriola, E, et al. LBA4 Randomized phase III study of first-line selpercatinib versus chemotherapy and pembrolizumab in RET fusion-positive NSCLC. Ann Oncol (2023) 34:S1303. doi:10.1016/j.annonc.2023.10.059
95. Zhou, C, Solomon, B, Loong, HH, Park, K, Pérol, M, Arriola, E, et al. First-line selpercatinib or chemotherapy and pembrolizumab in RET fusion-positive NSCLC. N Engl J Med (2023) 389:1839–50. doi:10.1056/NEJMoa2309457
96. FDA. FDA approves selpercatinib for lung and thyroid cancers with RET gene mutations or fusions (2021). Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-selpercatinib-lung-and-thyroid-cancers-ret-gene-mutations-or-fusions (Accessed January 24, 2024).
97. FDA. FDA approves pralsetinib for lung cancer with RET gene fusions (2020). Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-pralsetinib-lung-cancer-ret-gene-fusions (Accessed January 24, 2024).
98. EMA. Selpercatinib - summary of opinion (post authorisation) (2022). Available from: https://www.ema.europa.eu/en/documents/smop/chmp-post-authorisation-summary-positive-opinion-retsevmo-ii-0014-g_en.pdf (Accessed January 31, 2024).
99. EMA. Pralsetinib - summary of product characteristics (2024). Available from: https://www.ema.europa.eu/en/documents/product-information/gavreto-epar-product-information_en.pdf (Accessed January 31, 2024).
100. Griesinger, F, Curigliano, G, Thomas, M, Subbiah, V, Baik, CS, Tan, DSW, et al. Safety and efficacy of pralsetinib in RET fusion-positive non-small-cell lung cancer including as first-line therapy: update from the ARROW trial. Ann Oncol (2022) 33:1168–78. doi:10.1016/j.annonc.2022.08.002
101. Besse, B, Felip, E, Kim, ES, Clifford, C, Louie-Gao, M, Yagui-Beltran, A, et al. P87.02 AcceleRET lung: a phase 3 study of first-line pralsetinib in patients with RET-fusion+ advanced/metastatic NSCLC. J Thorac Oncol (2021) 16:S684. doi:10.1016/j.jtho.2021.01.1257
102. Chevallier, M, Borgeaud, M, Addeo, A, and Friedlaender, A Oncogenic driver mutations in non-small cell lung cancer: past, present and future. World J Clin Oncol (2021) 12:217–37. doi:10.5306/wjco.v12.i4.217
103. Abdayem, P, and Planchard, D Ongoing progress in BRAF-mutated non-small cell lung cancer. Clin Adv Hematol Oncol HO (2022) 20(1):662–672.
104. O’Leary, CG, Andelkovic, V, Ladwa, R, Pavlakis, N, Zhou, C, Hirsch, F, et al. Targeting BRAF mutations in non-small cell lung cancer. Transl Lung Cancer Res (2019) 8:1119–24. doi:10.21037/tlcr.2019.10.22
105. Harada, G, Yang, S-R, Cocco, E, and Drilon, A Rare molecular subtypes of lung cancer. Nat Rev Clin Oncol (2023) 20:229–49. doi:10.1038/s41571-023-00733-6
106. Hendriks, LE, Kerr, KM, Menis, J, Mok, TS, Nestle, U, Passaro, A, et al. Non-oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol Off J Eur Soc Med Oncol (2023) 34:358–76. doi:10.1016/j.annonc.2022.12.013
107. Davies, KD, Lomboy, A, Lawrence, CA, Yourshaw, M, Bocsi, GT, Camidge, DR, et al. DNA-based versus RNA-based detection of MET exon 14 skipping events in lung cancer. J Thorac Oncol (2019) 14:737–41. doi:10.1016/j.jtho.2018.12.020
108. Socinski, MA, Pennell, NA, and Davies, KD MET exon 14 skipping mutations in non-small-cell lung cancer: an overview of biology, clinical outcomes, and testing considerations. JCO Precis Oncol (2021) 5:653–63. doi:10.1200/PO.20.00516
109. FDA. List of cleared or approved companion diagnostic devices (in vitro and imaging tools) (2024). Available from: https://www.fda.gov/medical-devices/in-vitro-diagnostics/list-cleared-or-approved-companion-diagnostic-devices-in-vitro-and-imaging-tools (Accessed January 31, 2024).
110. Wolf, J, Seto, T, Han, J-Y, Reguart, N, Garon, EB, Groen, HJM, et al. Capmatinib in MET exon 14-mutated or MET-amplified non-small-cell lung cancer. N Engl J Med (2020) 383:944–57. doi:10.1056/NEJMoa2002787
111. ClinicalTrials.gov. Clinical study of oral cMET inhibitor INC280 in adult patients with EGFR wild-type advanced non-small cell lung cancer (geometry mono-1) (2023). Available from: https://clinicaltrials.gov/study/NCT02414139 (Accessed January 31, 2024).
112. Le, X, Sakai, H, Felip, E, Veillon, R, Garassino, MC, Raskin, J, et al. Tepotinib efficacy and safety in patients with MET exon 14 skipping NSCLC: outcomes in patient subgroups from the VISION study with relevance for clinical practice. Clin Cancer Res (2022) 28:1117–26. doi:10.1158/1078-0432.CCR-21-2733
113. ClinicalTrials.gov. Tepotinib phase II in NSCLC harboring MET alterations (VISION) (2023). Available from: https://clinicaltrials.gov/study/NCT02864992 (Accessed January 31, 2024).
114. Paik, PK, Felip, E, Veillon, R, Sakai, H, Cortot, AB, Garassino, MC, et al. Tepotinib in non-small-cell lung cancer with MET exon 14 skipping mutations. N Engl J Med (2020) 383:931–43. doi:10.1056/NEJMoa2004407
115. Xiong, W, Papasouliotis, O, Jonsson, EN, Strotmann, R, and Girard, P Population pharmacokinetic analysis of tepotinib, an oral MET kinase inhibitor, including data from the VISION study. Cancer Chemother Pharmacol (2022) 89:655–69. doi:10.1007/s00280-022-04423-5
116. Jebbink, M, de Langen, AJ, Boelens, MC, Monkhorst, K, and Smit, EF The force of HER2 - a druggable target in NSCLC? Cancer Treat Rev (2020) 86:101996. doi:10.1016/j.ctrv.2020.101996
117. Li, BT, Smit, EF, Goto, Y, Nakagawa, K, Udagawa, H, Mazières, J, et al. Trastuzumab deruxtecan in HER2-mutant non-small-cell lung cancer. N Engl J Med (2022) 386:241–51. doi:10.1056/NEJMoa2112431
118. Goto, K, Goto, Y, Kubo, T, Ninomiya, K, Kim, S-W, Planchard, D, et al. Trastuzumab deruxtecan in patients with HER2-mutant metastatic non-small-cell lung cancer: primary results from the randomized, phase II DESTINY-lung02 trial. J Clin Oncol (2023) 41:4852–63. doi:10.1200/JCO.23.01361
119. ClinicalTrials.gov. A study to investigate the efficacy and safety of trastuzumab deruxtecan as the first treatment option for unresectable, locally advanced/metastatic non-small cell lung cancer with HER2 mutations (2023). Available from: https://clinicaltrials.gov/study/NCT05048797 (Accessed January 31, 2024).
120. Demetri, GD, De Braud, F, Drilon, A, Siena, S, Patel, MR, Cho, BC, et al. Updated integrated analysis of the efficacy and safety of entrectinib in patients with NTRK fusion-positive solid tumors. Clin Cancer Res (2022) 28:1302–12. doi:10.1158/1078-0432.CCR-21-3597
121. Drilon, A, Tan, DSW, Lassen, UN, Leyvraz, S, Liu, Y, Patel, JD, et al. Efficacy and safety of larotrectinib in patients with tropomyosin receptor kinase fusion-positive lung cancers. JCO Precis Oncol (2022) 6:e2100418. doi:10.1200/PO.21.00418
122. Aggarwal, C, Marmarelis, ME, Hwang, W-T, Scholes, DG, McWilliams, TL, Singh, AP, et al. Association between availability of molecular genotyping results and overall survival in patients with advanced nonsquamous non-small-cell lung cancer. JCO Precis Oncol (2023) 7:e2300191. doi:10.1200/PO.23.00191
123. Aggarwal, C, Marmarelis, ME, Hwang, W-T, Scholes, DG, McWilliams, T, Singh, AP, et al. Association of comprehensive molecular genotyping and overall survival in patients with advanced non-squamous non-small cell lung cancer. J Clin Oncol (2022) 40:9022. doi:10.1200/JCO.2022.40.16_suppl.9022
124. Sequist, LV, Neal, JV, Jett, JR, and Ross, ME Personalized, genotype-directed therapy for advanced non-small cell lung cancer. UpToDate (2016).
125. Forde, PM, Spicer, J, Lu, S, Provencio, M, Mitsudomi, T, Awad, MM, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med (2022) 386:1973–85. doi:10.1056/NEJMoa2202170
126. Heymach, JV, Harpole, D, Mitsudomi, T, Taube, JM, Galffy, G, Hochmair, M, et al. Perioperative durvalumab for resectable non-small-cell lung cancer. N Engl J Med (2023) 389:1672–84. doi:10.1056/NEJMoa2304875
127. Wu, Y-L, Tsuboi, M, He, J, John, T, Grohe, C, Majem, M, et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N Engl J Med (2020) 383:1711–23. doi:10.1056/NEJMoa2027071
128. Tsuboi, M, Herbst, RS, John, T, Kato, T, Majem, M, Grohé, C, et al. Overall survival with osimertinib in resected EGFR-mutated NSCLC. N Engl J Med (2023) 389:137–47. doi:10.1056/NEJMoa2304594
129. Solomon, BJ, Ahn, JS, Dziadziuszko, R, Barlesi, F, Nishio, M, Lee, DH, et al. LBA2 ALINA: efficacy and safety of adjuvant alectinib versus chemotherapy in patients with early-stage ALK+ non-small cell lung cancer (NSCLC). Ann Oncol (2023) 34:S1295–6. doi:10.1016/j.annonc.2023.10.051
130. Solomon, BJ, Ahn, JS, Barlesi, F, Dziadziuszko, R, Nishio, M, Shaw, AT, et al. ALINA: a phase III study of alectinib versus chemotherapy as adjuvant therapy in patients with stage IB–IIIA anaplastic lymphoma kinase-positive (ALK+) non-small cell lung cancer (NSCLC). J Clin Oncol (2019) 37:TPS8569. doi:10.1200/JCO.2019.37.15_suppl.TPS8569
131. Gillespie, CS, Mustafa, MA, Richardson, GE, Alam, AM, Lee, KS, Hughes, DM, et al. Genomic alterations and the incidence of brain metastases in advanced and metastatic NSCLC: a systematic review and meta-analysis. J Thorac Oncol (2023) 18:1703–13. doi:10.1016/j.jtho.2023.06.017
132. Nishino, M, Soejima, K, and Mitsudomi, T Brain metastases in oncogene-driven non-small cell lung cancer. Transl Lung Cancer Res (2019) 8:S298–S307. doi:10.21037/tlcr.2019.05.15
133. Rangachari, D, Yamaguchi, N, VanderLaan, PA, Folch, E, Mahadevan, A, Floyd, SR, et al. Brain metastases in patients with EGFR-mutated or ALK-rearranged non-small-cell lung cancers. Lung Cancer Amst Neth (2015) 88:108–11. doi:10.1016/j.lungcan.2015.01.020
134. Tan, AC, and Tan, DSW Targeted therapies for lung cancer patients with oncogenic driver molecular alterations. JCO (2022) 40:611–625. doi:10.1200/JCO.21.01626
135. De Carlo, E, Bertoli, E, Del Conte, A, Stanzione, B, Berto, E, Revelant, A, et al. Brain metastases management in oncogene-addicted non-small cell lung cancer in the targeted therapies era. Int J Mol Sci (2022) 23:6477. doi:10.3390/ijms23126477
136. Le Rhun, E, Guckenberger, M, Smits, M, Dummer, R, Bachelot, T, Sahm, F, et al. EANO-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up of patients with brain metastasis from solid tumours. Ann Oncol (2021) 32:1332–47. doi:10.1016/j.annonc.2021.07.016
137. Thomas, NJ, Myall, NJ, Sun, F, Patil, T, Mushtaq, R, Yu, C, et al. Brain metastases in EGFR- and ALK-positive NSCLC: outcomes of central nervous system-penetrant tyrosine kinase inhibitors alone versus in combination with radiation. J Thorac Oncol (2022) 17:116–29. doi:10.1016/j.jtho.2021.08.009
138. NCCN. NCCN guidelines brain metastases version 1 (2023). Available from: https://www.nccn.org/professionals/physician_gls/pdf/cns.pdf (Accessed January 30, 2024).
Keywords: NSCLC, driver oncogenes, targeted therapy, central nervous system efficacy, molecular testing
Citation: Gálffy G, Morócz É, Korompay R, Hécz R, Bujdosó R, Puskás R, Lovas T, Gáspár E, Yahya K, Király P and Lohinai Z (2024) Targeted therapeutic options in early and metastatic NSCLC-overview. Pathol. Oncol. Res. 30:1611715. doi: 10.3389/pore.2024.1611715
Received: 31 January 2024; Accepted: 21 February 2024;
Published: 28 March 2024.
Edited by:
Maximilian Hochmair, Klinik Floridsdorf, AustriaCopyright © 2024 Gálffy, Morócz, Korompay, Hécz, Bujdosó, Puskás, Lovas, Gáspár, Yahya, Király and Lohinai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zoltán Lohinai, TE9ISU5BSS5aT0xUQU5AU0VNTUVMV0VJUy5IVQ==